News

Newswise — April 29, 2020 – Early reports of COVID-19 symptoms and the compelling need to quickly identify treatment options and curb the growing number of critically ill patients have led to erroneous and potentially dangerous comparisons between COVID-19 and other respiratory diseases like high altitude pulmonary edema, or HAPE. In “COVID-19 Lung Injury and High Altitude Pulmonary Edema: A False Equation with Dangerous Implications,” the authors urge clinicians to rely on scientific evidence to guide treatment. The paper was posted early online in the Annals of the American Thoracic Society.
There are some similarities between COVID-19 and HAPE as there are similarities between COVID-19 and other respiratory illnesses that cause respiratory failure: very low oxygen levels in the blood, significant difficulty breathing, the degree to which there is stiffness in the lungs, and abnormal findings on chest CT scans. However, there are fundamental differences between COVID-19 and HAPE.
“HAPE develops when people ascend to high altitude. The low oxygen levels in the atmosphere cause low oxygen levels in the air sacs of the lungs,” said Andrew Luks, MD, professor of medicine in the Division of Pulmonary, Critical Care and Sleep Medicine at Harborview Medical Center and the University of Washington. “In all people, this leads the blood vessels in the lungs to constrict and raises the blood pressure in the lungs (pulmonary artery pressure). In people who develop HAPE, this response is excessive. There is far too much vasoconstriction and far too great a rise in pulmonary artery pressure, all of which lead fluid to leak out of the blood vessels into the lung tissue, but this occurs with no inflammation.”
“In lung injury due to COVID-19, the virus attacks the cells that make up the air sacs of the lungs. This leads to a big inflammatory response that damages the air sacs (alveoli), leading fluid to leak out of the blood vessels even under much lower pressures, causes the alveoli to collapse, interferes with gas exchange and makes the lungs stiffer and harder to expand than normal. “
These fundamental differences necessitate different treatment approaches. While treatment with oxygen can resolve HAPE symptoms, oxygen alone is ineffective for the lung injury associated with COVID-19. Nifedpine and acetazolamide, two medications used to treat altitude sickness, can have dangerous consequences in COVID-19 patients.
“If given to a patient with lung injury due to COVID-19, it [nifedpine] has the potential to actually worsen oxygen levels in the blood and to lower systemic or whole body blood pressure,” said Dr. Luks.
Treating with acetazolamide can cause a host of problems, among them “fatigue of the diaphragm, causing the blood to become more acidic, and at high enough concentrations in the blood, impairing the transport and elimination of carbon dioxide, all of which will make patients even more short of breath.”
COVID-19 has affected how the medical community shares information and what the community is learning about the disease can change quickly. Clinicians and families are looking for data to help care for patients. Dr. Luks and his co-authors warn that without careful scrutiny, misinformation can quickly spread. Now more than ever, it is critical that clinicians rely on the data accumulated over time and scientific evidence related to treating acute lung injury.


Newswise — Amid the rapidly evolving global coronavirus disease 2019 (COVID-19) pandemic that has already had profound effects on public health and medical infrastructure across the globe, many questions remain about its impact on child health. New research published in the Journal of Clinical Virology indicates that the vulnerability of neonates and children and their role in the spread of the virus (severe acute respiratory syndrome coronavirus 2 [SARS-CoV-2]) should be included in preparedness and response plans.
According to lead author Kathleen M. Muldoon, Ph.D., Associate Professor, Anatomy at the Arizona College of Osteopathic Medicine at Midwestern University, the COVID-19 pandemic poses substantial and underappreciated risks to pregnant women, and perinatal infections endanger pregnancy outcomes. "Studies to date suggest that the virus can be transmitted to the fetus in utero," Dr. Muldoon says. "Although the evidence for infection is under debate, the possible routes for infection are such that infection control measures are required to protect newborns."
The potential for neonatal infection with the COVID-19 virus demands intensive study, including how viral pathology may or may not affect breast milk as the preferred method of infant nutrition, as well as the potential effects of vaccines on women of child-bearing age, unborn fetuses, and newborn infants.
"We are presenting the state of knowledge acquired to date about potential risks of transmission of SARS-CoV-2 to the fetus and newborn," continues Dr. Muldoon. "This research is timely because information regarding the potential routes of acquisition of SARS-CoV-2 infection in the prenatal and perinatal setting is of a high public health priority. Vaccines targeting women of reproductive age, and in particular pregnant patients, should be evaluated in clinical trials and should include the endpoints of neonatal infection and disease."
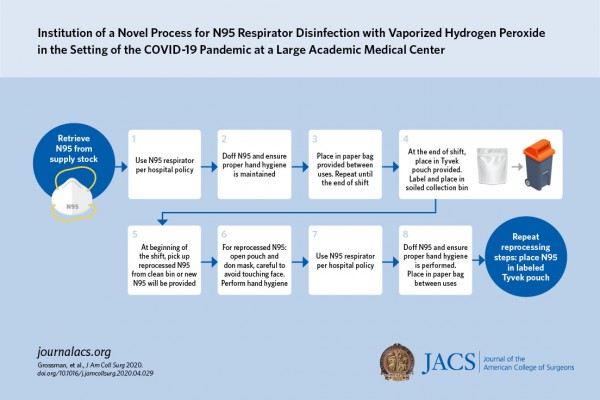
Newswise — CHICAGO (April 28, 2020): Amid shortages of personal protective equipment due to the Coronavirus Disease 2019 (COVID-19) pandemic, a St. Louis health care system has implemented a process to disinfect disposable N95 respirator masks that allows health care workers to reuse their own mask for up to 20 cycles. The novel disinfection process, developed in collaboration with Washington University School of Medicine, uses vaporized hydrogen peroxide and is described in an “article in press” on the Journal of the American College of Surgeons website in advance of print.
Test results from a pilot program at Barnes-Jewish Hospital and two other hospitals that are also part of BJC HealthCare, showed that the disinfection process kills germs from N95 masks while ensuring that the only person who touches the mask is the original mask wearer, study authors reported.
“Our primary outcome is safety for the health care worker,” said project leader and study coauthor Andrew Pierce, MHSA, director of supply plus at Barnes-Jewish. “We want to make it safer for team members who are at risk while taking care of patients with a known or possible COVID-19 diagnosis.”
Their program uses a disinfecting procedure first tested by Duke University researchers in 2016.1 However, the Barnes-Jewish process has a unique modification—an identification system that enables the hospital to return the sanitized mask to the same individual each time, said senior author Shaina Eckhouse, MD, FACS, assistant professor of surgery at Washington University School of Medicine, St. Louis. Dr. Eckhouse is part of the multidisciplinary team of university and hospital staff who developed the disinfection program.
This approach, according to the authors, increased employee acceptance of reusing what is normally a single-use N95 mask and helped ensure proper fit of the returned mask.
During the COVID-19 pandemic, the Centers for Disease Control and Prevention has recommended strategies for conserving personal protective equipment, including decontamination and reuse of N95 masks.2Almost half of U.S. health care facilities reported being nearly or completely out of N95 respirator masks, according to a March 27 survey conducted by the Association for Professionals in Infection Control and Epidemiology.3
In late March, before the program began, Barnes-Jewish had a low inventory of N95 masks—about a week’s worth—and no expectations for replenishment because of international shortages in hospital supply chains, according to Mr. Pierce.
How the process works
The disinfection process that has since been put into place begins at the end of a shift. A health care provider removes his or her N95 mask in that unit’s soiled utility room and places it in a sterilization pouch (Crosstex) made of breathable polyethylene fiber (Tyvek by DuPont) on one side. On the other side of the sealed pouch, the worker writes his or her name or employee ID number, hospital, department, and unit location and puts the pouch in the soiled collection bin.
A designated worker wearing proper protection collects the bins twice a day and takes them to a specially designed and sealed disinfection room—built in four days, according to Dr. Eckhouse. There the pouches are arranged, breathable side up, by clinical unit on wire racks. A hydrogen peroxide vapor generator (Bioquell Z-2), which Washington University already owned to decontaminate equipment, fills the room with the chemical.
After 4.5 hours of disinfection, a worker moves the racks of masks to another area that has a fan to offgas the hydrogen peroxide, where the masks stay until sensors record a zero reading. The pouches are returned to their respective units in a decontaminated bin, finishing a process that takes about seven hours, Mr. Pierce said.
Workers can wear their mask up to three weeks because past studies show that disinfection more than 20 times could alter the fit of the mask, he noted.
Since the program began April 1 in the Barnes-Jewish emergency department, it expanded in just two weeks to additional clinical departments and other hospitals in the system, which Mr. Pierce called “an immense achievement.”
“A welcome improvement”
Currently, Mr. Pierce said they are disinfecting 240 N95 masks a day and have the capability of disinfecting 1,500 masks daily.
Without the disinfection program, he said the health care system would need to discard a substantial amount of its respirator masks. Because of the disinfection, the hospitals now have enough masks to last for weeks.
“This program is a welcome improvement for extended usage of N95s during the shortage that we are facing,” Mr. Pierce said.
Dr. Eckhouse said other hospitals facing mask shortages can reproduce the disinfection program if they bring together experts in environmental health and safety, medicine, and facility management. “Having the infrastructure already in place would improve the ease of deploying an N95 disinfection process,” she stated.
Other study coauthors are Julie Grossman, MD; Jessica Mody, MHA; Jason Gagne, TS; Carol Sykora, CIC, FAPIC; Sena Sayood, MD; Susan Cook, PhD; Nirah Shomer, DVM, PhD; and Stephen Y. Liang, MD, MPHS.
“FACS” designates that a surgeon is a Fellow of the American College of Surgeons.
Image Credit: American College of SurgeonsCredit: Institution of a Novel Process for N95 Respirator Disinfection with Vaporized Hydrogen Peroxide in the Setting of the COVID-19 Pandemic at a Large Academic Medical Center
Janice M. Mehnert, MD
Newswise — New Brunswick, N.J. – April 27, 2020 – According to the National Cancer Institute, some 100,350 new cases of melanoma are expected in the U.S. this year with 6,850 deaths. Half of all melanoma cases have what is known as a BRAF mutation, and only about half of those treated with a BRAF-inhibitor (targeted therapy) respond to treatment.
As part of the SWOG Cancer Research Network and ECOG-ACRIN Cancer Research Group, investigators collaborated on a randomized phase 2 clinical trial examining the targeted therapy drugs dabrafenib and tremetinib in both continuous and intermittent treatment of patients with BRAF-mutated melanoma and found continuous dosing yields superior progression free survival.
Janice M. Mehnert, MD, director of the Phase I/Investigational Therapeutics Program at Rutgers Cancer Institute of New Jersey, and lead author Alain P. Algazi, MD, University of California San Francisco, are among the investigators. The research is being presented at the Opening Clinical Plenary Session of the virtual American Association for Cancer Research Annual Meeting, which was postponed as an in-person event this week due to COVID-19 concerns. Dr. Mehnert, who is also a medical oncologist in the Melanoma and Soft Tissue Oncology Program at Rutgers Cancer Institute and an associate professor at Rutgers Robert Wood Johnson Medical School, shares more about the work.
Q: What prompted you and your colleagues to focus on this work?
A: A Nature paper in 2011 (Das Thakur, et al.) demonstrated that in mice, withdrawal of therapy was able to induce a partial regression of melanoma tumors, and alternating periods with and without drug prolonged the time that the treatments worked. This led us to wonder whether this could be a more effective approach toward both delaying resistance to therapy and to ameliorating toxicity in patients treated with targeted therapy. In other words, could less therapy be more effective in patients?
Q: Tell us about the study and how it was conducted.
A: The 206 eligible patients all underwent an eight week lead in of drug therapy. Patients were then randomized to go forward on a continuous schedule or to an intermittent schedule of three weeks on therapy followed by five weeks off therapy. This was a large and rigorous study. Patients were drawn from 68 centers over five years. Seventy percent of the patients had not been treated with immune checkpoint inhibitors previously.
Q: What did you find?
A: In patients treated on this trial, the median progression-free survival was statistically significantly longer, 9.0 months from randomization, versus intermittent dosing at 5.5 months. There was no difference in overall survival between the groups at a follow up of two years.
Q: What are next steps related to this work?
A: On the schedules tested in this trial, continuous therapy is the optimal choice of targeted therapy. This is at odds with what was seen in the laboratory and with a few smaller studies that indicate treatment breaks may have benefit. It’s possible that different schedules with shorter drug-free intervals could have produced a different result, but it's hard to test this in patients because the drugs are metabolized differently in people than in mice. Given these results, continuous therapy remains the current standard of care.
This research was supported in part by grants from the National Institutes of Health/National Cancer Institute: CA180888, CA180819, CA180820, CA180850, CA239767, CA189808, CA46282, CA189858, CA189830, CA233230, CA189829, CA189954, CA189860, CA189822, CA189953, CA180834, CA189809, CA189957, and CA189958 (to SWOG), R35 CA197633 (to A.R.), and P01 CA244118 (to A.R. and R.S.L). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
A full author list, author disclosures and other information can be found at: https://www.abstractsonline.com/pp8/#!/9045/presentation/10595.

Newswise — The COVID-19 pandemic has hit some nursing homes especially hard – including in the hotspot state of Michigan.
Hundreds of deaths of residents in homes from Seattle to Boston have raised concerns about how well facilities are protecting the 1.3 million older Americans who live in them. Those concerns have prompted new federal and state requirements about testing and transparency.
But it might have been worse.
New data suggests that at least in Michigan, nursing homes that responded to a survey were far better prepared for this pandemic than they were for the last one. The study includes responses from130 nursing homes to a survey during the week the state announced its first documented case of COVID-19.
It shows that nearly all had a pandemic plan in place. That’s compared with just over half of the 280 nursing homes that answered the same survey in 2007. Nearly all said they now have at least one staff member in charge of pandemic preparedness.
The findings are reported in the Journal of the American Geriatrics Society by a team from the University of Michigan that has studied and worked to improve nursing home infection prevention for years.
Members of the team have several other recent publications with direct or indirect relevance to the COVID-19 pandemic, including putting forth recommendations for nursing homes and other housing facilities for older adults to use in planning how they will respond to pandemics such as COVID-19.
Lona Mody, M.D., M.Sc., a geriatrician at Michigan Medicine, U-M’s academic medical center, and the VA Ann Arbor Healthcare System, is senior author of both of the new publications. She’s a professor of internal medicine, the associate director for clinical and translational research at the U-M Geriatrics Center, and director of the Infection Prevention in Aging research group.
“Our nursing homes house some of the most vulnerable in our society,” says Mody. “This virus unfortunately is very contagious, the disease it causes has incredibly poor outcomes in older adults with comorbidities, and nursing homes are communal settings with shared spaces and resource limitations. This creates a perfect storm of sorts. Being novel, we learn as go and have to learn really quickly.”
Mody heads the PRIISM, or Preventing Resistance and Infection by Integrating Systems in Michigan, project, which partners with skilled nursing facilities, hospitals and public health agencies across the state to perform research and create and test education and training materials for nursing home staff. The program’s website has many free materials for use by nursing homes everywhere.
Pandemic planning
The new survey data show Michigan’s nursing homes have done a lot to prepare for pandemics since the last time the U-M team performed the survey. That previous survey was taken before the H1N1 influenza pandemic of 2009, but after the H5N1 “bird flu” pandemic of 2005 raised national awareness of the importance of pandemic preparedness. Mody and colleagues published pandemic preparedness guidance for nursing homes at that time.
In mid-March of this year, 85% of nursing homes said they had stockpiled supplies before COVID-19 hit, compared with 57% after the H5N1 pandemic. Most of those that had stockpiled supplies had focused on surgical masks, gloves and hand sanitizer. Less than half had stockpiled N95 respirator masks, which are recommended by national and global health authorities for health care workers performing certain types of care on a COVID-19 patient.
Still, 42% of the nursing homes that answered a question about COVID-19-specific concerns said they were worried about running short of personal protective gear.
“Although the size and severity of COVID-19 outbreaks in some nursing homes have taken everyone by surprise, just as so much about this pandemic has, in general nursing homes knew exactly what their challenges were going to be in a pandemic – PPE shortages, staff shortages and worries that they did not have the capacity to care for COVID patients after their hospital stay.”
Nearly all now said they had trained staff on how their facility would respond in a pandemic, up from 42% in 2007. But only one-third had conducted a pandemic drill. And Mody notes that nursing homes have a much higher rate of staff turnover than hospitals – meaning that training on infection prevention and pandemic response has to be offered whenever a new person joins the organization.
Michigan’s nursing homes appear to have gotten better connected to the broader health care system in the past decade, with significantly more saying they now have communication lines established with local hospitals and public health departments.
Many also said they were drawing COVID-19 guidance not just from the Centers for Disease Control and Prevention, but also from state and local health departments. Half also received guidance from their home’s corporate parent.
And while half of the nursing homes surveyed this year said they expected significant staff shortages due to COVID-19, most of them said they had a plan to deal with that. Most planned to ask existing clinical staff to work more hours, and to redeploy non-clinical staff. Two-thirds expected they’d need to require staff to work overtime.
The survey also explored the potential for nursing homes to relieve the burden on hospitals. In all, 82% said they’d be willing to take non-pandemic patients from overburdened hospitals now, compared with 53% in 2007. But the percent that said they’d be able to accept patients with the pandemic disease stayed the same, at one-third of responding homes.
Additional guidance
Mody and her colleagues John P. Mills, M.D. and Keith Kaye, M.D. from the U-M Division of Infectious Diseases recently published some recommendations regarding COVID-19 and older adults in the journal JCI Insight. Mody and Kaye are members of the U-M Institute for Healthcare Policy and Innovation.
They note that it’s not just nursing homes with long-term residents that need to be ready to care for vulnerable older adults during pandemics.
In fact, the trend over the past decade to use nursing homes more often for short-term stays by patients who have been discharged from a hospital, and to create state and local programs that allow older adults to ‘age in place’ instead of moving to nursing homes for the long-term, have led to potential gaps for pandemic responses to help older adults.
They call for policymakers to address those gaps, by creating pandemic-specific plans for community-dwelling older adults, especially those with health needs.
As for nursing homes, they recommend that in areas where COVID-19 is spreading widely in the community, facilities should take these steps, and others:
place patients with known or suspected disease in the same area of the facility, away from others
perform rapid COVID-19 tests on all patients, both short-stay and long-stay
screen healthcare workers and other staff for symptoms including checking temperatures
limit visitors and group activities
require everyone wear a surgical mask
require additional protective gear for clinical staff
The limits on group activities tie in to other research by Mody and her colleagues, published in JAGS in December.
That study sampled surfaces, and the hands of patients and staff, in the common areas and rehabilitation gyms with in nursing homes, and looked for drug-resistant bacteria that can cause dangerous infections. Though the team didn’t look for the presence of viruses in these areas, they did find that half of the samples taken in rehab gyms contained at least one type of bacteria that was resistant to several types of antibiotics.
In addition to stockpiling PPE and cleaning supplies, the recommend that nursing homes should use “burn calculators” to predict how quickly they’ll use those supplies based on their patient population.
If nursing homes and other residential facilities for older adults haven’t already done so, they should establish lines of communication with local health departments in advance of any outbreak of COVID-19 in their facility. They should also focus on staff retention, including providing for generous sick leave policies so that staff can stay home when ill, and hazard pay for those who can come to work.
And, the team says, nursing homes should make sure they have an infection prevention plan in place for staff when a patient has died of COVID-19.
Another gap in preparedness that the COVID-19 pandemic is revealing, Mody says, is a gap in communication with patients and their families. Keeping families informed, and enabling them to connect virtually with their loved ones when they can’t visit in person, is crucial, she says.
Florida Atlantic University
Joseph G. Ouslander, M.D., an internationally renowned geriatrician, a professor of geriatric medicine, and a senior advisor to the dean, FAU’s Schmidt College of Medicine.
Newswise — As the coronavirus disease (COVID-19) pandemic advances so does the uncertainty and evolution of the pandemic as it relates to nursing homes and long-term care facilities (LTCF). Early reports suggest the case fatality rate for those over 80, which constitutes nearly half of LTCF residents, is more than 15 percent. In areas where there is a shortage of ICU beds and respirators, even the most carefully thought out ethical approaches to rationing these resources will place older patients at a lower priority. LTCFs must be prepared to manage patients who have had or have COVID-19 infection.
In an editorial published in the Journal of the American Geriatric Society, Joseph G. Ouslander, M.D., an internationally renowned geriatrician, a professor of geriatric medicine, and a senior advisor to the dean at Florida Atlantic University’s Schmidt College of Medicine, provides key updates and resources for front-line nursing home staff and clinicians.
“Until more rapid COVID testing is available to enable us to test all nursing home patients and staff, cases of COVID-19 infection are likely to continue to increase in the long-term care facility setting,” said Ouslander. “To complicate matters, long-term care facilities will be asked to accept patients with possible or known COVID-19 from hospitals if the local or state government has not required the suspension of admissions during the presence of active COVID-19 cases.”
Ouslander recommends developing an emergency plan that addresses patient/resident placement and staffing considerations before a cluster infection or outbreak occurs; employing intensive infection control practices; behaving as if all patients and staff are potentially infected with the virus; and continuing to carefully screen staff, recognizing that some may be asymptomatic carriers of the virus and pass the screening.
In addition to restricting visitors, communal dining and cancelling other group activities, Ouslander advises providing therapy in the patient/resident room when feasible; if not, then safe social distancing should be used in therapy areas. Staff should wear plain surgical masks at all times and use N95 masks if available when performing high-risk procedures such as respiratory treatments. Full personal protective equipment (PPE) should be used when appropriate and available based on patient/resident symptoms and signs.
Staff who are quarantined based on symptoms and want to return to work must be tested to confirm they are not shedding the virus; returning health care workforce should be a priority for rapid testing. In addition, clinicians should monitor vital signs at least daily and more frequently if indicated; and even subtle changes in a patient’s condition should be taken seriously and further evaluated when clinically indicated.
Because LTCF patients/residents cannot have visitors or participate in group activities, their isolation may have adverse effects on their mental health. Morale of staff may also be affected. Experience in China suggests that half or more of health care workers treating patients with COVID-19 infection had symptoms of depression, anxiety, insomnia or distress. Ouslander suggests that LTCFs provide as much psychosocial care and support as feasible and use social media and video phone call options. Grief counseling for families and staff, as well as assistance with burial arrangements may be needed.
In the United States, of the approximately 1.2 million registered nurses employed outside of hospital settings, 24 percent are ages 55 to 64 years and 5 percent are age 65 years or older. Of the approximately 1.2 million physicians, an estimated 230,000 (20 percent) are ages 55 to 64 years and an estimated 106,000 (9 percent) are age 65 years or older. Many hospitals and health care systems are developing strategies to use these health professionals in productive ways that may not necessarily involve direct patient contact. The U.S. Centers for Medicare and Medicaid Services has issued many waivers that could help bolster the health care workforce and the capacity of the nation’s health care system to care for older COVID-19 patients.
“During this challenging and unprecedented pandemic of our lifetimes, we should be thankful for all of the front-line nursing home staff and clinicians who are risking their health and that of their families to care for the most vulnerable among us,” said Ouslander. “Shortages of these professionals are anticipated, and the aging of our health care workforce makes many of us even more susceptible to acquiring COVID-19 and its complications. We all have a role to play, and we should support our geriatric health care workforce, our patients, and their families in whatever ways we can contribute to meet this daunting challenge.”
Newswise — Rockville, Md. (April 16, 2020)—A new review suggests that higher-than-normal levels of an enzyme involved in blood clot prevention may be a common risk factor for developing COVID-19—a respiratory disease caused by the novel coronavirus SARS-CoV-2—in some populations. The review is published in Physiological Reviews.
People with diabetes, high blood pressure and heart, lung or kidney disease have a higher risk of developing COVID-19. In addition, people with preexisting medical conditions typically become sicker when infected with SARS-CoV-2 than those in otherwise good health. Research has found that one of the leading causes of death from COVID-19 is hemorrhage or bleeding disorders and that one of the characteristics of the disease is overactivity of the system responsible for removing blood clots (hyperfibrinolysis).
Elevated levels of plasminogen and plasmin have been found to be a common factor in people with diabetes and preexisting heart, lung and kidney conditions. Plasminogen is an inactive substance in the blood. When substances in the cells of the blood vessels activate plasminogen, it generates plasmin, an enzyme that removes blood clots from the blood. Higher-than-normal levels of both of these chemicals can lead to severe bleeding.
Studies report that more than 97% of people hospitalized with COVID-19 have increased levels of D-dimer, a protein in the blood that is produced when a blood clot dissolves. D-dimer levels are associated with the amount of virus detected in the body and continue to rise as the severity of COVID-19 increases. This is particularly true in people who develop the often-fatal complication of acute respiratory distress syndrome (ARDS). “In contrast, D-dimer levels decreased to control levels in [COVID-19] survivors or non-ARDS patients,” the review’s authors wrote. “The time [period] for the elevated D-dimer [to go] down in mild [cases] or survivors is dependent. Generally, it takes at least one week for mild [cases] but longer for severe patients,” explained Hong-Long Ji, MD, PhD, corresponding author of the review.
“Measurements of plasmin(ogen) levels and its enzymatic activity may be important biomarkers of disease severity” in people with COVID-19, the authors wrote. In addition, treating hyperfibrinolysis “may prove to be a promising strategy for improving the clinical outcomes of patients with [additional medical] conditions,” they added.
Read the full article, “Elevated plasmin(ogen) as a common risk factor for COVID-19 susceptibility,” published in Physiological Reviews. This article is part of a special, freely accessible coronavirus-related collection of articles published in APS journals.
Physiology is the study of how molecules, cells, tissues and organs function in health and disease. Established in 1887, the American Physiological Society (APS) was the first U.S. society in the biomedical sciences field. The Society represents 9,000 members and publishes 15 peer-reviewed journals with a worldwide readership.

Newswise — PHILADELPHIA — A new trial led by the Perelman School of Medicine at the University of Pennsylvania will evaluate whether the use of medications to treat high blood pressure affect outcomes among patients who are prescribed the medication and hospitalized with COVID-19. As part of the multi-center, international trial called REPLACE COVID, investigators will examine whether ACE inhibitors (ACEI) or Angiotensin Receptor Blockers (ARBs)—two classes of medications to treat high blood pressure—help to mitigate complications or lead to more severe symptoms and worse outcomes. The study (NCT04338009) is enrolling patients now.
Through the trial, investigators will randomly assign patients who are hospitalized with COVID-19 to either stop or continue taking their prescribed medication. The team will closely monitor the patients to evaluate the effect of temporarily stopping the therapy. Julio A. Chirinos, MD, PhD, an associate professor of Cardiovascular Medicine, and Jordana B. Cohen, MD, MSCE, an assistant professor in the division of Renal-Electrolyte and Hypertension, are the study’s co-principal investigators.
“While some data suggests patients with underlying health conditions, like heart disease and high blood pressure, have a higher risk of developing a more severe form of COVID-19, we don’t know whether ACE inhibitors or ARBs are beneficial or harmful,” Chirinos said. “There’s an urgent need to understand how these medications may alter the disease course so we can better guide our treatment for patients who are prescribed these therapies and infected with COVID-19.”
High blood pressure, defined as a top reading of at least 130 or a bottom one of 80, affects nearly half of American adults. If left untreated, the condition increases one’s risk for severe complications, including heart attack and stroke. More than one-third of people with high blood pressure are prescribed ACEIs or ARBs. Past research has shown that these medications may enhance the virus’ ability to bind to cells in the body. However, separate studies have found that the medications may, in fact, result in an improved response in the kidney, lung, and heart to protect against the virus.
For this trial, investigators plan to enroll 152 patients who are hospitalized with a suspected diagnosis of COVID-19 and who already use one of the medications. The team, which also includes Thomas C. Hanff, MD, MPH, a Cardiovascular Medicine fellow at Penn, will perform the study on a pragmatic intent-to-treat basis, meaning clinicians can change the dose or discontinue the medications if there is a compelling clinical reason.
Ultimately, investigators aim to develop a global risk score that ranks patient outcomes based on four factors: time to death, the number of days supported by mechanical ventilation or extracorporeal membrane oxygenation (ECMO), length of time on renal replacement therapy, and a modified sequential organ failure assessment score.
“Many people are changing their usual medical management right now based on limited or incomplete information,” Cohen said. “Until we have high quality evidence, we recommend that patients continue to take these medications as prescribed unless they are told to stop them by their medical provider.”
Given the study’s expedited timeframe, investigators are pursuing a variety of funding mechanisms. The team also established a social fundraising campaign to help support the study.
Jesse L. Chittams, managing director of the Biostatistics Analysis Core at the University of Pennsylvania, is also an investigator on the study.

Photo by James Zanewicz
The new COVID-19 testing being done at the medical school will save time from having to ship samples to the state lab in Baton Rouge. The goal is to do about 100 tests a day, with results available within 24 hours.
Newswise — Tulane University has added a second avenue for COVID-19 testing, this one taking place at a Tulane School of Medicine repurposed research lab where results can be processed within a day. The test is identical to the PCR test being used by the Centers for Disease Control (CDC) and is another way that Tulane is working to ease the testing crisis and stop the spread of COVID-19, which has hit the New Orleans area especially hard.Earlier this week, a laboratory based at Tulane Medical Center in partnership with LSU and UMC-LCMC began conducting a different new test for COVID-19 that can yield results within four hours. Researchers at the HCA-TMC Laboratory ran its first set of tests using the Cobas 6800 analyzer over the weekend and is now capable of running nearly 200 tests a day on patients at both Tulane Medical Center and University Medical Center. The testing being done at the medical school will save time from having to ship samples to the state lab in Baton Rouge, where because of demand, results can take days, rather than hours, to obtain. “Tulane’s efforts could help more quickly triage patients to the appropriate section of the hospital, speed up recruitment into clinical trials for interested patients, and even, over time, provide the ability to determine whether viral loads are affected by various interventions,” said Dr. Dahlene Fusco, an infectious disease specialist at Tulane University School of Medicine. “This information is crucial in our understanding of how to best treat patients.”The School of Medicine test was developed by Tulane virologist Bob Garry and his team in collaboration with Drs. Xiao-Ming Yin and Di Tian in the Department of Pathology. It is based on the PCR (Polymerase Chain Reaction) test being used by the CDC, which determines a positive or negative diagnosis through a nasal swab. For now, the test is available only to members of the Tulane medical community who show symptoms of COVID-19, such as coughing, respiratory struggles and fever. They include patients, health care providers, faculty, staff, residents and students. The goal is to do about 100 tests a day, with results available within 24 hours. Eventually, Tulane hopes to double the number of tests and, if possible, extend their availability to the community.Garry, who played an integral role in test development during the Lassa and Ebola crises, said Tulane’s ability to offer the test is a significant achievement, given the complex and ever-changing regulatory environment under which the nation’s medical community is operating.“Because it’s an in-house test, we don’t need to send samples to a central lab to wait for the result,” Garry said. “It’s not rocket science but it does take a supply chain which is challenging but getting better.” Garry facilitated the test in collaboration with the Pathology Department, which has validated and is administering the test in a lab certified by the Clinical Laboratory Improvement Amendments (CLIA) which ensures quality lab testing. Patrice Delafontaine, executive dean of the School of Medicine, said the availability of CLIA-certified lab in pathology was essential in getting the COVID-19 testing lab up and running. “Dr. Lee Hamm (dean of the School of Medicine) and I felt it was critical to organize this effort very quickly,” he said, “and the extraordinary expertise in virology at Tulane, in particular through Bob Garry and his program, provided the most efficient method to get this done.”

Numerical data sometimes reveal facts that are otherwise concealed within an onslaught of information from an overwhelming number of sources. Prof. Ron Milo and research student Yinon Bar-On of the Weizmann Institute of Science’s Department of Plant and Environmental Sciences, together with American colleagues Prof. Rob Phillips of Caltech and Dr. Avi Flamholz of the University of California, Berkeley, have now employed an original research method to organize the flood of coronavirus information in an orderly framework.
The scientists examined hundreds of studies from around the world. The first stage of the project required the scientists to understand the different measurement and estimation methods so that they could coordinate and translate all the findings into the same “language” – a complex task requiring great care. The scientists’ experience helped them in this task, as they translated and consolidated a wealth of data and findings that they accumulated in previous studies: the number of cells in the human body, biomass distribution on Earth, and more. (For example, see: http://book.bionumbers.org/.)
The research was fast-tracked to publication in the journal eLife. One of the interesting findings highlighted by the collected data is the similarity between the coronavirus genome and the genome of other viruses. For example, the genome of the coronavirus is:
96% identical to a coronavirus genome that infects bats
91% identical to a coronavirus genome that infects scaly anteaters (pangolins)
80% identical to the SARS virus that erupted about two decades ago
55% identical to the MERS virus that erupted eight years ago
50% identical to the coronavirus that causes “common colds”
The scientists also present numerical data on the coronavirus’s attachment to various organs in the body (bronchi, lungs, different types of cells, and more).
The study presents the number of copies and other quantitative features of virus “targets,” which are relevant for developing vaccines and pharmaceuticals that block the virus’s ability to adhere to and penetrate a human cell.
An additional part of the team’s research relates to the virus’s mutation accumulation rate. This value is related to the chance (risk) that the virus will bypass vaccines developed against it – and return to attack humans. The coronavirus’s mutation accumulation rate is relatively slow compared to influenza viruses; Prof. Milo cautiously estimates that this may indicate that drugs and vaccines developed by scientists will be more durable in curbing this virus over time.
Prof. Ron Milo’s research is supported by the Mary and Tom Beck – Canadian Center for Alternative Energy Research, which he heads; the Zuckerman STEM Leadership Program; Dr. and Mrs. Brian Altman; the Larson Charitable Foundation New Scientist Fund; the Ullmann Family Foundation; Dana and Yossie Hollander; and the European Research Council. Prof. Milo is the incumbent of the Charles and Louise Gartner Professorial Chair.
The Weizmann Institute of Science in Rehovot, Israel, is one of the world’s top-ranking multidisciplinary research institutions. The Institute’s 3,800-strong scientific community engages in research addressing crucial problems in medicine and health, energy, technology, agriculture, and the environment. Outstanding young scientists from around the world pursue advanced degrees at the Weizmann Institute’s Feinberg Graduate School. The discoveries and theories of Weizmann Institute scientists have had a major impact on the wider scientific community, as well as on the quality of life of millions of people worldwide.