News
Newswise — Lawrenceville, NJ, USA—May 26, 2020—Value in Health, the official journal of ISPOR—the professional society for health economics and outcomes research, announced today the publication of a series of articles focused on methods for moving from the evaluation of precision medicine into practice and policy. The series was published in the May 2020 issue of Value in Health.
“Precision medicine is an emerging approach for disease treatment and prevention that takes into account individual variability in genes, environment, and lifestyle,” said Guest Editor Kathryn A. Phillips, PhD, Center for Translational and Policy Research on Personalized Medicine, University of California at San Francisco, San Francisco, CA, USA. “This approach allows clinicians and researchers to predict more accurately which treatments and prevention strategies for a particular disease will work in which groups of people.”
The themed section highlights next-generation sequencing technologies, which are the fastest-growing type of precision medicine technology. These technologies include panels that test multiple genes for a single indication, whole exome sequencing tests that evaluate the entire exome (coding regions of the genome), and whole genome sequencing tests that evaluate the entire genome.
In her introductory editorial, “Methods for Moving the Evaluation of Precision Medicine Into Practice and Policy,” Phillips provides historical perspective and introduces the other 5 articles in the series:
“Being Precise About Precision Medicine: What Should Value Frameworks Incorporate to Address Precision Medicine? A Report of the Personalized Precision Medicine Special Interest Group,” by Eric Faulkner,Anke-Peggy Holtorf, Surrey Walton, Christine Y. Liu, Hwee Lin, Eman Bilta,j Diana Brixner, Charles Barr, Jennifer Oberg, Gurmit Shandhu, Uwe Siebert, Susan R. Snyder, Simran Tiwana, John Watkins, Maarten J. IJzerman, and Katherine Payne
“Use of Real-World Evidence in US Payer Coverage Decision-Making for Next-Generation Sequencing–Based Tests: Challenges, Opportunities, and Potential Solutions,” by Patricia A. Deverka, Michael P. Douglas, and Kathryn A. Phillips, PhD
“Insights From a Temporal Assessment of Increases in US Private Payer Coverage of Tumor Sequencing From 2015 to 2019,”by Julia R. Trosman, Michael P. Douglas, Su-Ying Liang, Christine B. Weldon, Allison W. Kurian, Robin K. Kelley, and Kathryn A. Phillips
“Quantifying Downstream Healthcare Utilization in Studies of Genomic Testing,” by Zoë P. Mackay, Dmitry Dukhovny, Kathryn A. Phillips, Alan H. Beggs, Robert C. Green, Richard B. Parad, and Kurt D. Christensen
“Addressing Challenges of Economic Evaluation in Precision Medicine Using Dynamic Simulation Modeling,” by Deborah A. Marshall, Luiza R. Grazziotin, Dean A. Regier, Sarah Wordsworth, James Buchanan, Kathryn A. Phillips, and Maarten Ijzerman
“Much progress has been made in developing and applying methods to evaluate precision medicine,” said Phillips. “Nevertheless, new tests such as minimally invasive liquid biopsies and emerging approaches such as artificial intelligence and machine learning platforms will continue to require the development and adaptation of methods used to assess the value of precision medicine. The collective efforts of a society like ISPOR can bring together the wide range of disciplines and stakeholders that will be needed to continue to evolve the methods and approaches used to assess precision medicine.”

SCIENTISTS ENGINEER MOSQUITOES THAT RESIST MALARIA PARASITE W/COMBINATION OF ANTI-PARASITE MOLECULES

Newswise — Anopheles mosquitoes that have been genetically engineered with multiple anti-malaria molecules, acting at different stages of the malaria life cycle, are strongly resistant to the parasite that causes malaria and are unlikely to lose that resistance quickly, according to a study from scientists at Johns Hopkins Bloomberg School of Public Health.
The study, published May 13 in the journal Science Advances, is an early-stage laboratory demonstration that will be followed by further testing. The findings suggest that releasing such mosquitoes in areas where malaria is endemic could dramatically reduce local, mosquito-borne transmission of malaria to humans for prolonged periods.
“We were able to achieve a very efficient suppression of infection in the mosquitoes by combining antimalarial proteins that would be difficult for the parasite to evade,” says senior author George Dimopoulos, PhD, professor in the Department of Molecular Microbiology and Immunology at the Bloomberg School. Malaria is caused by Plasmodium parasites, which infect certain mosquito species and can be transmitted among humans and other mammals via mosquito “bites.” The disease continues to be one of the world’s top public health threats, accounting for about 200 million clinical cases and 400,000 deaths per year, mostly children under age five in sub-Saharan Africa.
Decades of efforts towards a malaria vaccine have resulted so far in just one product. In a large clinical trial, the vaccine reduced serious malaria cases by only about 30 percent—far from the near-complete protection provided by modern vaccines against most viruses and bacteria. Antimalaria drugs are available but have significant side effects, provide incomplete protection against malaria symptoms, and do not prevent human infection by the parasite.
A newer approach, inspired by the emergence of genetic engineering technology, is to create populations of mosquitoes that carry genes conferring resistance to malaria parasites. In theory, releasing such mosquitoes into the wild would lead to the spread of those genes in local mosquito populations, a consequent decline in Plasmodium infection in the mosquitoes, and thus a decline in mosquito-borne transmission of malaria to humans.
Scientists since the late 1990s have reported numerous strategies for engineering malaria resistance into mosquitoes. However, the malaria parasite is a relatively large organism compared to bacteria and viruses; it has thousands of genes with which it can evolve ways to survive and keep proliferating in its mosquito or mammalian hosts despite attacks from antimalarial drugs or other factors.
In the new study, Dimopoulos and his team engineered Anopheles mosquitoes with a combination of multiple antimalarial effector proteins that block infection. This strategy minimizes the parasite’s chances of developing resistance to the effector proteins and resume the parasite’s ability to be transmitted to and infect humans. One element of the strategy was a single artificial gene, or transgene, encoding five proteins that are known to kill malaria parasites; these included Shiva 1, a toxin from spider venom; Scorpine, a toxin from scorpion venom; and Melittin, a toxin from bee venom.
The scientists combined this five-in-one transgene with another transgene encoding an antibody-plus-toxin molecule that homes in on the late, sporozoite stage of the parasite. As an alternative strategy, the scientists combined the antibody-toxin transgene with a transgene that stimulates the early mosquito immune defense against malaria infection. The transgenes in each case were designed to become active whenever the host mosquito had a blood meal.
The scientists found that both of these combination approaches succeeded in greatly suppressing infection of mosquitoes by Plasmodium falciparum, the parasite species that causes most of the serious cases of malarial illness and nearly all malaria deaths. The degree of suppression was more than enough, in principle, to eliminate or greatly reduce malaria transmission to humans by such engineered mosquitoes.
Mosquitoes carrying the foreign, insect-venom genes were found to have suffered a slight “fitness cost” in terms of reduced lifespan, which in the wild would result in the loss of these genes from the mosquito gene pool over time. However, in practice, antimalarial transgenes can be engineered into mosquitoes with so-called “gene drives” that overcome normal mechanisms of heredity and essentially force the antimalarial transgenes into a high percentage of mosquito offspring. This strategy, if proven successful, could one day convert a malaria-transmitting mosquito population to one that can’t transmit the parasite.
Dimopoulos and his team now plan to follow up by integrating their antimalarial transgenes into gene drive systems and by modeling the effects on malaria transmission of releasing these engineered mosquitoes in the wild.
“Ultimately, transgenic mosquito -based strategies like ours probably will advance to the point that there will be test releases of engineered mosquitoes under controlled conditions,” Dimopoulos says. “Once those studies show there is no danger, then I think that people will be more open to this type of approach to malaria prevention.“Versatile transgenic multi-stage effector-gene combinations for Plasmodium falciparum suppression in Anopheles” was written by Yuemei Dong, Maria L. Simões, and George Dimopoulos.
Support for the research was provided by the National Institutes of Health (R01AI061576, R01AI061576, R01AI122743, R01AI122743), the Bloomberg Philanthropies, and the Johns Hopkins Malaria Research Institute.
Cellular processes happen every day in humans and plants, such as homeostasis and photosynthesis
The cells involved in the process are so complex it’s challenged human understanding, especially how they act in different environments
A bioelectrical conceptualisation of cells could be the key to researching how cells operate, researchers at the School of Life Sciences, University of Warwick argue
If the genetics, physics and physiology can be grounded on bioelectrical conceptualisation of cells it could have implications for research in conditions related to cellular processes
Newswise — We use cells to breathe, to moderate body temperature, to grow and many other every day processes, however the cells in these processes are so complex its left scientists perplexed into how they develop in different environments. Researchers from the University of Warwick say future research needs to look into the bioelectrical composition of cells for answers.
Cellular processes happen every day for survival, form homeostasis to photosynthesis and anaerobic respiration to aerobic respiration. However the complexity of cells has fascinated and challenged human understanding for centuries.
It’s cellular “machinery” responsible for key functions have been the focus of biology research, and despite previous research exploring the molecular and genetic basis of these processes showing unprecedented insights, we still can’t fully understand and predict cell behaviour when challenged to different conditions.
In particular, the basis of heterogeneity in single-cell behaviour and the initiation of many different metabolic, transcriptional or mechanical responses to environmental stimuli remain largely unexplained.
Researchers from the School of Life Sciences at the University of Warwick have today, the 20th May had the paper ‘Bioelectrical understanding and engineering of cell biology’ published in the journal Royal Society Interface, in which they have gone beyond the status quo of understanding cell behaviours, and argue a combination of genetics, physics and physiology can be grounded on a bioelectrical conceptualisation of cells.
They argue that a bioelectrical view can provide predictive biological understanding, which can open up novel ways to control cell behaviours by electrical and electrochemical means, setting the stage for the emergence of bioelectrical engineering.
Dr Orkun Soyer, from the School of Life Sciences at the University of Warwick comments:
“When looking at the underlying chemistry of this “machinery” it is easy to recognise the importance of electricity in biological phenomena.
“Here we advocate that the understanding of cells as electrical entities will pave the way to fully understand, predict and modulate cellular function. When cellular functions are understood it could have a huge impact on healthcare, as conditions related to, for example, homeostasis such as heart failure or diabetes, could have new treatments researched if we can manipulate the bioelectricity in the cells.”
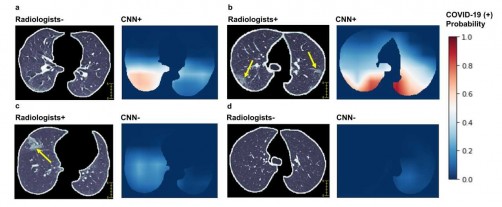
Newswise — (New York, NY – May 19, 2020) – Mount Sinai researchers are the first in the country to use artificial intelligence (AI) combined with imaging, and clinical data to analyze patients with coronavirus disease (COVID-19). They have developed a unique algorithm that can rapidly detect COVID-19 based on how lung disease looks in computed tomography (CT scans) of the chest, in combination with patient information including symptoms, age, bloodwork, and possible contact with someone infected with the virus. This study, published in the May 19 issue of Nature Medicine, could help hospitals across the world quickly detect the virus, isolate patients, and prevent it from spreading during this pandemic.
“AI has huge potential for analyzing large amounts of data quickly, an attribute that can have a big impact in a situation such as a pandemic. At Mount Sinai, we recognized this early and were able to mobilize the expertise of our faculty and our international collaborations to work on implementing a novel AI model using CT data from coronavirus patients in Chinese medical centers. We were able to show that the AI model was as accurate as an experienced radiologist in diagnosing the disease, and even better in some cases where there was no clear sign of lung disease on CT,” says one of the lead authors, Zahi Fayad, PhD, Director of the BioMedical Engineering and Imaging Institute (BMEII) at the Icahn School of Medicine at Mount Sinai. “We’re now working on how to use this at home and share our findings with others—this toolkit can easily be deployed worldwide to other hospitals, either online or integrated into their own systems.”
This research expands on a previous Mount Sinai study that identified a characteristic pattern of disease in the lungs of COVID-19 patients and showed how it develops over the course of a week and a half.The new study involved scans of more than 900 patients that Mount Sinai received from institutional collaborators at hospitals in China. The patients were admitted to 18 medical centers in 13 Chinese provinces between January 17 and March 3, 2020. The scans included 419 confirmed COVID-19-positive cases (most either had recently traveled to Wuhan, China, where the outbreak began, or had contact with an infected COVID-19 patient) and 486 COVID-19-negative scans. Researchers also had patients’ clinical information, including blood test results showing any abnormalities in white blood cell counts or lymphocyte counts as well as their age, sex, and symptoms (fever, cough, or cough with mucus). They focused on CT scans and blood tests since doctors in China use both of these to diagnose patients with COVID-19 if they come in with fever or have been in contact with an infected patient.
The Mount Sinai team integrated data from those CT scans with the clinical information to develop an AI algorithm. It mimics the workflow a physician uses to diagnose COVID-19 and gives a final prediction of positive or negative diagnosis. The AI model produces separate probabilities of being COVID-19-positive based on CT images, clinical data, and both combined. Researchers initially trained and fine-tuned the algorithm on data from 626 out of 905 patients, and then tested the algorithm on the remaining 279 patients in the study group (split between COVID-19-positive and negative cases) to judge the test’s sensitivity; higher sensitivity means better detection performance. The algorithm was shown to have statistically significantly higher sensitivity (84 percent) compared to 75 percent for radiologists evaluating the images and clinical data. The AI system also improved the detection of COVID-19-positive patients who had negative CT scans. Specifically, it recognized 68 percent of COVID-19-positive cases, whereas radiologists interpreted all of these cases as negative due to the negative CT appearance. Improved detection is particularly important to keep patients isolated if scans don’t show lung disease when patients first present symptoms (since the previous study showed that lung disease doesn’t always show up on CT in the first few days) and COVID-19 symptoms are often nonspecific, resembling a flu or common cold, so it can be difficult to diagnose.
CT scans are not widely used for diagnosis of COVID-19 in the United States; however, Dr. Fayad explains that imaging can still play an important role.
“Imaging can help give a rapid and accurate diagnosis—lab tests can take up to two days, and there is the possibility of false negatives—meaning imaging can help isolate patients immediately if needed, and manage hospital resources effectively. The high sensitivity of our AI model can provide a ‘second opinion’ to physicians in cases where CT is either negative (in the early course of infection) or shows nonspecific findings, which can be common. It’s something that should be considered on a wider scale, especially in the United States, where currently we have more spare capacity for CT scanning than in labs for genetic tests,” said Dr. Fayad, who is also a Professor of Diagnostic, Molecular and Interventional Radiology at the Icahn School of Medicine at Mount Sinai.
“This study is important because it shows that an artificial intelligence algorithm can be trained to help with early identification of COVID-19, and this can be used in the clinical setting to triage or prioritize the evaluation of sick patients early in their admission to the emergency room,” says Matthew Levin, MD, Director of the Mount Sinai Health System’s Clinical Data Science Team, and a member of the Mount Sinai COVID Informatics Center. “This is an early proof concept that we can apply to our own patient data to further develop algorithms that are more specific to our region and diverse populations.”
Mount Sinai researchers are now focused on further developing the model to find clues about how well patients will do based on subtleties in their CT data and clinical information. They say this could be important to optimize treatment and improve outcomes.
Xueyan Mei, a trainee in the Graduate School of Biological Sciences at the Icahn School of Medicine at Mount Sinai, and Yang Yang, PhD, Assistant Professor of Radiology at the Icahn School of Medicine at Mount Sinai, also contributed to this work.
Image credit: BioMedical Engineering and Imaging Institute (BMEII) at the Icahn School of Medicine at Mount Sinai
Journal of the American College of Surgeons article highlights early research on blood clotting evaluation work that may help identify and treat dangerous complications of the infection
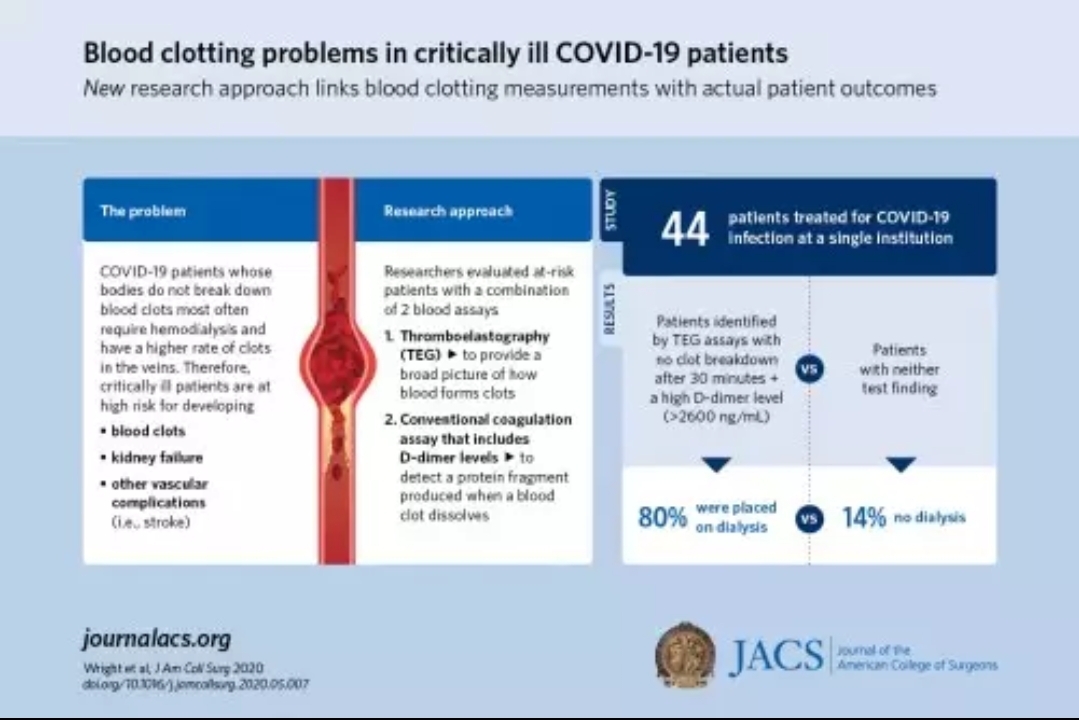
Newswise — CHICAGO (May 15, 2020): When researchers from the University of Colorado Anschutz Medical Campus, Aurora, used a combination of two specific blood-clotting tests, they found critically ill patients infected with Coronavirus Disease 2019 (COVID-19) who were at high risk for developing renal failure, venous blood clots, and other complications associated with blood clots, such as stroke. Their study, which was one of the first to build on growing evidence that COVID-19-infected patients are highly predisposed to developing blood clots, linked blood clotting measurements with actual patient outcomes. The research team is now participating in a randomized clinical trial of a drug that breaks down blood clots in COVID-19-infected patients. “This is an early step on the road to discovering treatments to prevent some of the complications that come with this disease,” said Franklin Wright, MD, FACS, lead author of the research article and an assistant professor of surgery at the University of Colorado School of Medicine. Their research is published as an “article in press” on the Journal of the American College of Surgeons website ahead of print.
Patients who are critically ill regardless of cause can develop a condition known as disseminated intravascular coagulation (DIC). The blood of these patients initially forms many clots in small blood vessels. The body’s natural clotting factors can form too much clot or eventually not be able to effectively form any clot leading to issues of both excessive clotting and excessive bleeding. However, in patients with COVID-19 the clotting appears to be particularly severe and—as evidenced by case studies in China and elsewhere*—clots in COVID-19 patients do not appear to dissipate, explained Dr. Wright.
Trauma acute care surgeons and intensive care physicians who treat trauma, transplant, and cardiothoracic surgery patients at UCHealth University of Colorado Hospital saw the potential of using a specialized coagulation test to examine clotting issues in COVID-19 patients. Thromboelastography (TEG) is a whole blood assay that provides a broad picture of how an individual patient’s blood forms clots, including how long clotting takes, how strong clots are, and how soon clots break down. TEG is highly specialized and used primarily by surgeons and anesthesiologists to evaluate the efficiency of blood clotting; it is not widely used in other clinical settings. “The COVID pandemic is opening doors for multidisciplinary collaboration so trauma acute care surgeons and intensivists can bring the tools they use in their day-to-day lives and apply them in the critical care setting to new problems,” Dr. Wright said.
The researchers evaluated outcomes for all patients who had a TEG assay as part of their treatment for COVID-19 infection as well as other conventional coagulation assays, including ones that measure D-dimer levels. D-dimer is a protein fragment that is produced when a blood clot dissolves. D-dimer levels are elevated when large numbers of clots are breaking down.
A total of 44 patients treated for COVID-19 infection between March 22 and April 20 were included in the analysis. Those whose bodies were not breaking down clots most often required hemodialysis and had a higher rate of clots in the veins. These patients were identified by TEG assays showing no clot breakdown after 30 minutes and a D-dimer level greater than 2600 ng/mL. Eighty percent of patients with both affirmative test findings were placed on dialysis compared with 14 percent who tested for neither finding. Patients with affirmative test findings also had a 50 percent rate of venous blood clots compared with 0 percent for those patients with neither finding.
“These study results suggest there may be a benefit to early TEG testing in institutions that have the technology to identify COVID-19 patients who may need more aggressive anticoagulation therapy to prevent complications from clot formation,” Dr. Wright said.
A clinical trial of one form of treatment is already underway. The Denver Health and Hospital Authority is leading a multi-center study that includes UCHealth University of Colorado Hospital, National Jewish Health-St Joseph Hospital, Beth Israel Deaconess Medical Center, and Long Island Jewish Hospital in conjunction with Genentech, Inc., enrolling patients with COVID-19 infection in a randomized clinical trial of tissue plasminogen activator (tPA). This drug is a natural anticoagulant that was approved by the U.S. Food and Drug Administration in 1996 for the treatment of diseases associated with clotting disorders, such as heart attack, stroke, and pulmonary embolism. The trial will assess the efficacy and safety of intravenous tPA in improving respiratory function and management of patients with aggressive blood clotting.
“This study suggests that testing whole blood clotting measurements may allow physicians to identify and treat patients with COVID-19 more effectively to prevent complications and encourage further research into therapies to prevent blood clots in these patients,” Dr. Wright said.
Dr. Wright’s associates in this study include: Thomas O. Vogler, PhD; Ernest E. Moore, MD, FACS; Hunter B. Moore, MD, PhD; Max V. Wohlauer, MD; Shane Urban, BSN, RN; Trevor L. Nydam, MD, FACS; Peter K. Moore, MD; and Robert C. McIntyre Jr., MD, FACS.
Photo credit:
American College of Surgeons
Fibrinolysis Shutdown Correlation with Thromboembolic Events in Severe COVID-19 Infection
200 YEARS AFTER FLORENCE NIGHTINGALE’S BIRTH, NURSES ARE ON THE FRONT LINE, BATTLING A SILENT KILLER

Newswise — It seems fitting that on the 200th anniversary of Florence Nightingale’s birth, nurses are being celebrated the world over for their bravery, kindness, skills and sacrifice.
The International Day of the Nurse coincides with the worst pandemic in a century. COVID-19 has already infected more than four million people and killed over 280,000, including a rising tally of healthcare workers.
Being on the front line of the pandemic has been bittersweet for the global nursing profession, according to Professor Marion Eckert, Director of the Rosemary Bryant AO Research Centre and Professor of Cancer Nursing in South Australia.
“2020 is the International Year of the Nurse and the Midwife,” says Prof Eckert. “We should be planning celebrations this year but instead we are battling a silent killer, leaving not only ourselves vulnerable but our families, too.”
Nurses comprise the largest single workforce in Australia, numbering around 380,000 in this country and 28 million worldwide, eclipsing every other profession.
Their role is important in normal circumstances; right now, it is pivotal to containing a disease that is crippling health systems and economies across the globe.
“The value of nurses has never been more prominent. Every day they are going to work, not knowing if they are going to be infected, or inadvertently infect others. It becomes all encompassing, yet they have to put that aside and focus on the task at hand – caring for others.”
Prof Eckert says the community recognition and appreciation has helped nurses cope in these difficult months, particularly in countries where the coronavirus has left an enormous toll.
“People clapping in the streets and their neighbourhoods, supermarkets opening early specifically for healthcare workers, and simple gestures like cafes giving free coffees to nurses are all making a difference,” she says.
And despite the stresses currently facing the nursing profession, there are opportunities emerging from this crisis. The fast tracking of tele health services is allowing nurses to connect with remote and rural communities in ways they have never done before.
The newfound respect for nurses and interest in their role also bodes well for future investment in nursing education and research.
In recent days, UniSA’s Rosemary Bryant AO Research Centre has seized the initiative to establish a clinical research network to collaborate on translational nursing and midwifery research across Australia and New Zealand.
The centre’s namesake has welcomed the move, saying the COVID-19 pandemic has identified some important gaps in nurses’ and midwives’ education.
Dr Rosemary Bryant AO, Australia’s first Commonwealth Chief Nursing and Midwifery Director, and former Executive Director of the Royal College of Nursing Australia, says nursing research receives scant funding compared to health research overall.
“Nurses comprise the largest workforce in the country and there is a critical need for research in that area alone,” Dr Bryant says. “It is also timely to look at changes to both the content and length of nursing courses to ensure we are educating them adequately for future challenges.”
Describing nurses as “the glue that holds the health system together,” Dr Bryant says in her 50 plus years in the profession, she has seen a gradual shift in community perception towards nurses.
“Salaries and working conditions have both improved in recent decades, reflecting the higher status of nurses, but there are subtle shifts, too. Patients have always thanked doctors, but now they are thanking nurses as well. And while people have always been aware of the role that nurses play, this has been heightened during this pandemic.”
Dr Bryant says Florence Nightingale, acknowledged as the world’s founder of modern nursing, would be “blown away” by the global efforts of the nursing fraternity to defeat COVID-19.
“It was her work in the Crimean War that led to modern infection control and the saving of so many lives. She was the first person to demonstrate that cleanliness and distancing hospital beds were the key to fighting disease.”
Two hundred years later, Nightingale’s legacy is crystal clear.

Gastrointestinal symptoms, coupled with a fever or history of exposure to COVID-19, could indicate coronavirus infection in children
Newswise — Children suffering from sickness and diarrhea, coupled with a fever or history of exposure to coronavirus, should be suspected of being infected with COVID-19, recommends a new study published in Frontiers in Pediatrics.
The research also suggests that the gastrointestinal symptoms first suffered by some children hints at potential infection through the digestive tract, as the type of receptors in cells in the lungs targeted by the virus can also be found in the intestines.
"Most children are only mildly affected by COVID-19 and the few severe cases often have underlying health issues. It is easy to miss its diagnosis in the early stage, when a child has non-respiratory symptoms or suffers from another illness," says author of this study, Dr. Wenbin Li, who works at the Department of Pediatrics, Tongji Hospital, Wuhan, China.
He continues, "Based on our experience of dealing with COVID-19, in regions where this virus is epidemic, children suffering from digestive tract symptoms, especially with fever and/or a history of exposure to this disease, should be suspected of being infected with this virus."
In this study, Li and his colleagues detail the clinical features of children admitted to hospital with non-respiratory symptoms, which were subsequently diagnosed with pneumonia and COVID-19.
"These children were seeking medical advice in the emergency department for unrelated problems, for example, one had a kidney stone, another a head trauma. All had pneumonia confirmed by chest CT scan before or soon after admission and then confirmed to have COVID-19. While their initial symptoms may have been unrelated, or their COVID-19 symptoms were initially mild or relatively hidden before their admission to hospital, importantly, 4 of the 5 cases had digestive tract symptoms as the first manifestation of this disease."
By highlighting these cases, Li hopes that doctors will use this information to quickly diagnose and isolate patients with similar symptoms, which will aid early treatment and reduce transmission.
The researchers also link the children's gastrointestinal symptoms, which have been recorded in adult patients, to an additional potential route of infection.
Li explains, "The gastro-intestinal symptoms experienced by these children may be related to the distribution of receptors and the transmission pathway associated with COVID-19 infection in humans. The virus infects people via the ACE2 receptor, which can be found in certain cells in the lungs as well as the intestines. This suggests that COVID-19 might infect patients not only through the respiratory tract in the form of air droplets, but also through the digestive tract by contact or fecal-oral transmission."
While COVID-19 tests can occasionally produce false positive readings, Li is certain all these five children were infected with the disease, but he cautions that more research is needed to confirm their findings.
"We report five cases of COVID-19 in children showing non-respiratory symptoms as the first manifestation after admission to hospital. The incidence and clinical features of similar cases needs further study in more patients."

Newswise — Children, teens and young adults are at greater risk for severe complications from COVID-19 than previously thought and those with underlying health conditions are at even greater risk, according to a study coauthored by a Rutgers researcher.
The study, published in JAMA Pediatrics, is the first to describe the characteristics of seriously ill pediatric COVID-19 patients in North America.
“The idea that COVID-19 is sparing of young people is just false,” said study coauthor Lawrence C. Kleinman, professor and vice chair for academic development and chief of the Department of Pediatrics’ Division of Population Health, Quality and Implementation Science at Rutgers Robert Wood Johnson Medical School. “While children are more likely to get very sick if they have other chronic conditions, including obesity, it is important to note that children without chronic illness are also at risk. Parents need to continue to take the virus seriously.”
The study followed 48 children and young adults – from newborns to 21 years old — who were admitted to pediatric intensive care units (PICUs) in the United States and Canada for COVID-19 in March and April. More than 80 percent had chronic underlying conditions, such as immune suppression, obesity, diabetes, seizures or chronic lung disease. Of those, 40 percent depended on technological support due to developmental delays or genetic anomalies.
More than 20 percent experienced failure of two or more organ systems due to COVID-19, and nearly 40 percent required a breathing tube and ventilator. At the end of the follow-up period, nearly 33 percent of the children were still hospitalized due to COVID-19, with three still requiring ventilator support and one on life support. Two of the children admitted during the three-week study period died.
“This study provides a baseline understanding of the early disease burden of COVID-19 in pediatric patients,” said Hariprem Rajasekhar, a pediatric intensivist involved in conducting the study at Robert Wood Johnson Medical School’s Department of Pediatrics. “The findings confirm that this emerging disease was already widespread in March and that it is not universally benign among children.”
The researchers said they were “cautiously encouraged” by hospital outcomes for the children studied, citing the 4.2 percent mortality rate for PICU patients compared with published mortality rates of up to 62 percent among adults admitted to ICUs, as well as lower incidences of respiratory failure.
Kleinman noted that doctors in the New York metropolitan area are seeing what appears to be a new COVID-related syndrome in children.
“Although our data collection for this study has ended, we continue to develop collaborations with colleagues in our region and across the country to try to understand these more severe complications,” he said, citing concerns such as heart failure and the Kawasaki disease–like condition termed pediatric multi-system inflammatory syndrome as examples.

Newswise — A new study shows that a financial incentive can dramatically increase the number of emergency department physicians trained to prescribe a potentially life-saving medication that prevents patients from fatal opioid overdose.
Led by researchers in Emergency Medicine at the Perelman School of Medicine at the University of Pennsylvania (Penn Medicine), the study showed that, at its start, just 6 percent of eligible physicians across three different emergency departments (EDs) had the proper training to prescribe the medication buprenorphine. But by offering reimbursement for training and a $750 incentive, 89 percent of physicians in those EDs were fully trained six weeks later. The study was published this month in Annals of Emergency Medicine.
“This study shows how enthusiastically emergency physicians embraced the opportunity to obtain this certification, which speaks to the shifting national conversation surrounding opioid use disorder and the importance of meeting patients where they are,” said Sean Foster, MD, an assistant professor of Emergency Medicine and the director of Quality Improvement in Emergency Medicine at Penn Presbyterian Medical Center. “This also gives a ‘playbook’ of sorts to any leaders and administrators who may be looking for ways to get their group trained.”
Buprenorphine is an “agonist” drug, meaning that it soothes the brain’s cravings for opioids and has a ceiling effect on their toxic effects, preventing fatal overdose. By prescribing buprenorphine, ED doctors provide a “bridge” from acute care to longer term care that can include everything from counseling to continuing medications that will better support recovery.
A post-intervention survey for the study and actual buprenorphine prescribing data showed that in addition to having such a high rate of those trained, which is called getting an “X waiver,” the physicians used their certification fairly quickly. Roughly 65 percent of respondents reported that they either administered or prescribed buprenorphine within the five months of their training.
“Buprenorphine is underutilized because of a lack of X waivered providers and the stigma associated with taking this medication, with some suggesting it’s ‘replacing one drug with another,’” said Jeanmarie Perrone, MD, a professor of Emergency Medicine and the director of the new Center for Addiction Medicine and Policy at Penn Medicine. “’However, buprenorphine has been shown to unequivocally decrease opioid overdose deaths and decrease the transmission of infections such as hepatitis C or HIV.”
To get their X waiver, physicians must devote an entire day to training, which can be difficult to schedule amid their many responsibilities. It also wasn’t very common until recently for the emergency department to be the venue for buprenorphine prescription. The incentive and reimbursement ($750 and $200, respectively, in this case) as well as changing attitudes toward the medication seem to make the decision to get an X waiver much easier for the 67 physicians it was offered to.
Of the three emergency department locations, two actually achieved a 100 percent X waiver rate. This included one site that went from zero X waivers to all of its ED doctors having one., and another site that went from just three of its physicians having X waivers to 26.
The variation in X waiver rates by site was not directly studied, but Foster thinks he knows why one site did particularly well.
“That particular site has the most readily available access to certified recovery specialists, who are absolutely essential in making the bridge from the emergency department to the doctor’s office,” Foster explained. “They are also incredible advocates for the patients while in the emergency department, and can help patients work through any hesitation they may have about participating in these treatments.”
A related project at Penn Medicine called CORE that utilized both certified recovery specialists and the promotion of X waiver training resulted in 7 out of 10 patients being in active recovery a month after visiting the emergency department. Typical national numbers without buprenorphine prescriptions hover around 1 in 10.
While $750 could be seen as steep for some health systems, the post-intervention survey in this study revealed that two-thirds of respondents would have felt moved to get their X waiver even if the incentive was $500 or less.
Moving forward, to explore more ways to introduce buprenorphine use, the study team hopes to explore the effectiveness of “mini X waivers,” a shorter training course.
“This study targets emergency physicians to ensure that they better understand the way buprenorphine works in order to administer it for opioid withdrawal symptoms in the emergency department,” Perrone said. “In this setting, the X waiver certification is not required but it can still be a bridge to getting patients into treatment.”
Other authors on this study included Kathleen Lee, MD; Christopher Edwards, MD; Arthur Pelullo; Utsha Khatri, MD; and Margaret Lowenstein, MD.

Newswise — Despite the use of personal protective equipment (PPE), reports show that many health care workers contracted the coronavirus disease (COVID-19), which raises substantial concerns about the effectiveness of the PPE. Highly sought after PPE used in hospitals and other health care settings is critical in ensuring the safety of those on the frontline of COVID-19, but only if they are used properly.
A physician from Florida Atlantic University’s Schmidt College of Medicine and collaborators from the University of Arizona College of Medicine -Tucson and the Indiana University School of Medicine conducted a novel training technique to reinforce the importance of using proper procedures to put on and take off PPE when caring for patients during the pandemic. Researchers were able to vividly demonstrate how aerosol-generating procedures can lead to exposure of the contagion with improper use of PPE.
To detect contamination, Patrick G. Hughes, D.O., lead author, director of FAU’s emergency medicine simulation program and an assistant professor of Integrated Medical Science, FAU’s Schmidt College of Medicine, and collaborators, used a nontoxic fluorescent solution during a PPE training session for health care staff. They placed a highlighter refill in a warm water bath for 15 minutes to create a fluorescent solution, which is only visible under ultraviolet light.
For the experiment, published in the journal Medical Education, the researchers instructed health care staff to put on PPE, which included a cap, gown, surgical gloves, eye protection, face shield and N95 mask. In order to conserve vital PPE, supplies were wiped off and reused for multiple trainings. After health care staff in the study put on their PPE, they went in to a room to care for a simulated patient sprayed down with the invisible simulated contagion. In addition, the researchers added the fluorescent solution to a simulated albuterol nebulizer treatment, which was given to the mannequins during the scenario (not in a negative pressure room).
After completing the simulated case, the health care staff remained in their PPE and were taken to another room, where the lights were turned off prior to removing their PPE. Turning off the lights enabled the identification of widespread simulated contagion on the PPE, both on the gloves and gowns from directly touching the simulated patient and on the face shields and masks from the aerosolized solution. The researchers used a black light flashlight to examine each health care worker and to identify the presence of any fluorescent solution.
Following the flashlight examination, the health care staff completely removed their PPE. Researchers discovered the presence of fluorescent solution on the health care staff’s skin, which represented an exposure to the contagion and indicated that they made an error while putting on or taking off their PPE.
Results from the experiment revealed that the most common error made by the health care staff was contaminating the face or forearms during PPE removal. In contrast, those who put on and took off their PPE according to guidelines had no signs of the fluorescent contagion on their skin or face.
“This training method allows educators and learners to easily visualize any contamination on themselves after they fully remove their personal protective equipment,” said Hughes. “We can make immediate corrections to each individual’s technique based on visual evidence of the exposure.”
By providing health care staff with visual evidence of protection during patient encounters with high-risk aerosol-generating procedures, this innovative training method is helping to inspire trust in their training and PPE.
“This experiment demonstrated that following PPE training improves workplace safety and decreases the risk of transmission,” said Hughes. “This simulation-based approach provides an efficient, low-cost solution that can be implemented in any hospital.”
Hughes also conducted this training technique with FAU’s emergency medicine resident physicians in the medical school’s Clinical Skills Simulation Center, which uses high-tech and high-fidelity patient mannequins in life-like hospital and emergency room settings. The center applies sophisticated simulation and trainer technologies to educate medical students, resident physicians, registered nurses, first responders, certified nursing assistants, home health aides and community health care providers. The center has created models of hospital rooms, patient examination, and emergency rooms for simulated patient treatment. The rooms are fully equipped with hospital beds, gurneys or exam tables, monitors, IV poles, defibrillators, blood pressure cuffs, simulated oxygen ports, otoscopes and ophthalmoscopes and all equipment and supplies required to respond to medical and nursing interventions, including emergencies.
The simulation team uses high fidelity wireless, full body male and female mannequins. The simulators track all actions taken and all pharmacological agents given to the patients. If incorrect drugs or dosages are administered, the high-fidelity patient responds exactly as a human patient would respond. Preceptors and session facilitators provide guidance during the simulations.
Study co-authors are Kate E. Hughes, D.O., emergency medicine, University of Arizona College of Medicine -Tucson; and Rami A. Ahmed, D.O., emergency medicine, Indiana University School of Medicine, Indianapolis.
Photo Credit: Rami A. Ahmed, D.O.