News
Newswise — BIRMINGHAM, Ala. –
Women live longer than men.
This simple statement holds a tantalizing riddle that Steven Austad, Ph.D., and Kathleen Fischer, Ph.D., of the University of Alabama at Birmingham explore in a perspective piece published in Cell Metabolism on June 14.
“Humans are the only species in which one sex is known to have a ubiquitous survival advantage,” the UAB researchers write in their research review covering a multitude of species. “Indeed, the sex difference in longevity may be one of the most robust features of human biology.”
Though other species, from roundworms and fruit flies to a spectrum of mammals, show lifespan differences that may favor one sex in certain studies, contradictory studies with different diets, mating patterns or environmental conditions often flip that advantage to the other sex. With humans, however, it appears to be all females all the time.
“We don’t know why women live longer,” said Austad, distinguished professor and chair of the UAB Department of Biology in the UAB College of Arts and Sciences. “It’s amazing that it hasn’t become a stronger focus of research in human biology.”
Evidence of the longer lifespans for women includes:• The Human Mortality Database, which has complete lifespan tables for men and women from 38 countries that go back as far as 1751 for Sweden and 1816 for France. “Given this high data quality, it is impressive that for all 38 countries for every year in the database, female life expectancy at birth exceeds male life expectancy,” write Austad and Fischer, a research assistant professor of biology.• A lifelong advantage. Longer female survival expectancy is seen across the lifespan, at early life (birth to 5 years old) and at age 50. It is also seen at the end of life, where Gerontology Research Group data for the oldest of the old show that women make up 90 percent of the supercentenarians, those who live to 110 years of age or longer.• The birth cohorts from the mid-1800s to the early 1900s for Iceland. This small, genetically homogenous country — which was beset by catastrophes such as famine, flooding, volcanic eruptions and disease epidemics — provides a particularly vivid example of female survival, Austad and Fischer say. Over that time, “life expectancy at birth fell to as low as 21 years during catastrophes and rose to as high as 69 years during good times,” they write. “Yet in every year, regardless of food availability or pestilence, women at the beginning of life and near its end survived better than men.”• Resistance to most of the major causes of death. “Of the 15 top causes of death in the United States in 2013, women died at a lower age-adjusted rate of 13 of them, including all of the top six causes,” they write. “For one cause, stroke, there was no sex bias, and for one other, Alzheimer’s disease, women were more at risk.”
Cell Metabolism invited Austad to contribute this perspective paper, “Sex differences in lifespan.”
Austad first became interested in the topic when Georgetown University asked him to lecture on it in 2003. Although lab models like the roundworm C. elegans, the fruit fly Drosophila melanogaster and the mouse Mus musculus are intensively used in scientific studies, people in those fields are not very aware of how longevity patterns by sex can vary according to genetic backgrounds, or by differences in diet, housing or mating conditions, Austad says.
Those uncontrolled variables lead to different results in longevity research. A survey of 118 studies of laboratory mice by Austad and colleagues in 2011 found that 65 studies reported that males outlived females, 51 found that females outlived males, and two showed no sex difference.
But if variables are carefully controlled, mice may prove to be a useful model to study sex differences in the cellular and molecular physiology of aging, Austad and Fischer write.
This understanding will be helpful as researchers start to develop drugs for human use that affect aging, Austad says. “We may be able to develop better approaches,” he said. “There is some complicated biology underlying sex differences that we need to work on.”
Differences may be due to hormones, perhaps as early as the surge in testosterone during male sexual differentiation in the uterus. Longevity may also relate to immune system differences, responses to oxidative stress, mitochondrial fitness or even the fact that men have one X chromosome (and one Y), while women have two X chromosomes.
But the female advantage has a thorn.
“One of the most puzzling aspects of human sex difference biology,” write Austad and Fischer, “something that has no known equivalent in other species, is that for all their robustness relative to men in terms of survival, women on average appear to be in poorer health than men through adult life.”
This higher prevalence of physical limitations in later life is seen not only in Western societies, they say, but also for women in Bangladesh, China, Egypt, Guatemala, India, Indonesia, Jamaica, Malaysia, Mexico, the Philippines, Thailand and Tunisia.
One intriguing explanation for this mortality-morbidity paradox is a possible connection with health problems that appear in later life. Women are more prone to joint and bone problems, such as osteoarthritis, osteoporosis and back pain, than are men. Back and joint pain tends to be more severe in women, and this could mean chronic sleep deprivation and stress. Thus, the sex differences in morbidity could be due to connective tissue maladies in women, and connective tissue in humans is known to respond to female sex hormones.
But this is just one of several plausible hypotheses for the mystery of why women live longer, on average, than men.

Newswise — Washington, DC —
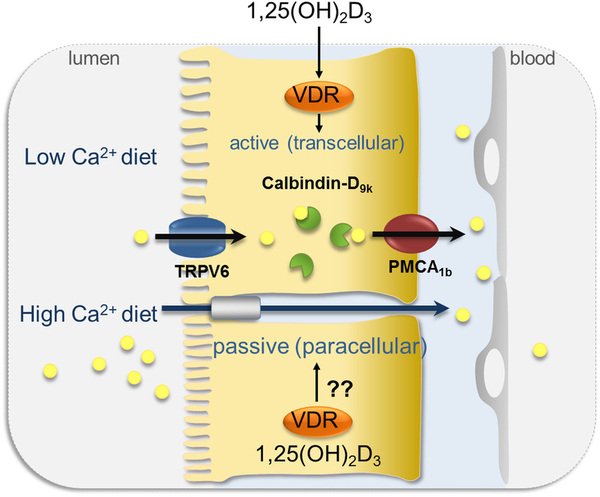
Measuring intestinal calcium absorption may help to identify individuals who are prone to develop kidney stones, according to a study appearing in an upcoming issue of the Clinical Journal of the American Society of Nephrology(CJASN).
Individuals with hypercalciuria have kidneys that put out higher levels of calcium in urine than normal, which increases their risk of developing kidney stones. Only a portion of hypercalciuric individuals will develop stones, however, and there are no criteria to distinguish them from those who remain free of stones.
To look for such distinguishing factors, Giuseppe Vezzoli, MD (San Raffaele Scientific Institute, in Milan, Italy) and his colleagues evaluated absorption of calcium in the first part of the small intestine as well as urinary excretion of calcium in 172 hypercalciuric stone formers and 36 hypercalciuric patients without a history of kidney stones.
The researchers found that both absorption and excretion of calcium were faster in hypercalciuric stone formers than in hypercalciuric patients without a history of stones.
“To our knowledge this is the first study comparing calcium metabolism in hypercalciuric patients with or without calcium stones,” said Dr. Vezzoli. “Its findings identify a characteristic of calcium metabolism that may predispose hypercalciuric patients to calcium stone formation, and highlight the role of intestinal absorption in stone formation.”
Study co-authors include Lorenza Macrina, MD, Alessandro Rubinacci, MD, Donatella Spotti, MD, and Teresa Arcidiacono, MD.
Disclosures: The study was supported by grants from the Italian Ministry of University and Scientific Research and from the San Raffaele Scientific Institute.
The article, entitled “Intestinal calcium absorption among hypercalciuric patients with or without calcium kidney stones will appear online athttp://www.cjasn.asnjournals.org/ on June 9, 2016, doi:10.2215/CJN.10360915.
The content of this article does not reflect the views or opinions of The American Society of Nephrology (ASN). Responsibility for the information and views expressed therein lies entirely with the author(s). ASN does not offer medical advice. All content in ASN publications is for informational purposes only, and is not intended to cover all possible uses, directions, precautions, drug interactions, or adverse effects. This content should not be used during a medical emergency or for the diagnosis or treatment of any medical condition. Please consult your doctor or other qualified health care provider if you have any questions about a medical condition, or before taking any drug, changing your diet or commencing or discontinuing any course of treatment. Do not ignore or delay obtaining professional medical advice because of information accessed through ASN. Call 911 or your doctor for all medical emergencies.Founded in 1966, and with nearly 16,000 members, the American Society of Nephrology (ASN) leads the fight against kidney disease by educating health professionals, sharing new knowledge, advancing research, and advocating the highest quality care for patients.# # #
Newswise —
Prostate cancer patients may soon have a new option to treat their disease: laser heat. UCLA researchers have found that focal laser ablation – the precise application of heat via laser to a tumor – is both feasible and safe in men with intermediate risk prostate cancer.
The Phase 1 study, published June 10 in the peer-reviewed Journal of Urology, found no serious adverse effects or changes in urinary or sexual function six months after the procedure. The technique uses magnetic resonance imaging, or MRI, to guide the insertion of a laser fiber into cancerous tumors. When heated, the laser destroys the cancerous tissue.
A follow-up study, presented in a poster presentation at the American Urology Association meeting in May, showed the potential to transfer this treatment for the first time into a clinic setting, using a special device (Artemis) that combines both MRI and ultrasound for real-time imaging. The Artemis device arrived at UCLA in 2009. Since then, 2000 image-fusion biopsies have been performed – the most in the U.S. - and this large experience has paved the way for treatment to be done in the same way.
If the laser technique, known as MRI-guided focal laser ablation, proves effective in further studies -- especially using the new MRI-ultrasound fusion machine -- it could improve treatment options and outcomes for men treated for such cancers, said study senior author Dr. Leonard Marks, a professor of urology and director of the UCLA Active Surveillance Program. Historically, prostate cancer has been treated with surgery and radiation, which can result in serious side effects such as erectile dysfunction and urinary incontinence.
“Our feeling was that if you can see prostate cancer using the fusion MRI and can put a needle in the spot to biopsy it, why not stick a laser fiber in the tumor the same way to kill it,” Marks said. “This is akin to a lumpectomy for breast cancer. Instead of removing the whole organ, target just the cancer inside it. What we are doing with prostate cancer now is like using a sledgehammer to kill a flea.”
Up until now, capturing an image of a prostate cancer has been difficult because prostate tissue and tumor tissue are so similar. Precise, non-invasive surgical treatment has proved difficult as a result.
As the Journal of Urology study shows, however, MRI improves the ability of physicians to perform precise, laser-based treatment. The new fusion-imaging method improves it even further, providing real-time ultrasound that more clearly delineates the tumor. By combining laser ablation with this fusion-imaging technique, the potential of laser ablation grows enormously.
Previous research at UCLA has demonstrated the value of using the same fusion imaging technique to perform biopsies to diagnose prostate cancers in men with rising PSA who had multiple negative conventional biopsies. Such biopsies are usually “blind,” meaning physicians take a tissue sample based on what they believe is the location of a possible tumor.
The new Journal of Urology study provides proof of principle that laser ablation can be done safely and effectively with MRI. In this case, eight men underwent ablation while in an MRI machine. Although none had serious side effects, longer-term follow-up is needed, as is a continued assessment of appropriate treatment margins to ensure cure, the researchers said.
The second study tested the fusion-MRI procedure on 11 men in a clinical setting. That study found the procedure was well -tolerated under local anesthesia and resulted in no side effects. At four months follow-up, there were no changes in urinary or sexual function.
“This focal therapy provides a middle ground for men to choose between radical prostatectomy and active surveillance, between doing nothing and losing the prostate,” Marks said. “This is a new and exciting concept for prostate cancer treatment.”
The laser treatment is not yet approved for use in prostate cancer by the U.S. Food and Drug Administration.
“I think we were so successful in this effort because of the experience we gained doing the targeted biopsies,” Marks said. “That allowed us to go from biopsy to treatment.”
The studies were funded through private philanthropy and by a grant from Medtronic.
For more than 50 years, the urology specialists at UCLA have continued to break new ground and set the standards of care for patients suffering from urological conditions. In collaboration with research scientists, UCLA’s internationally renowned physicians are pioneering new, less invasive methods of delivering care that are more effective and less costly. UCLA’s is one of only a handful of urology programs in the country that offer kidney and pancreas transplantation. In July of 2015, UCLA Urology was ranked third in the nation by U.S. News & World Report. For more information, visit http://www.urology.ucla.edu/.

Newswise — DENVER –
Twenty to 50 percent of Americans suffer from acute insomnia each year, defined as difficulty falling asleep or staying asleep, three or more nights per week, for between two weeks and three months. Roughly 10 percent of Americans experience chronic insomnia lasting longer than three months. The effects of chronic insomnia (and/or sleep loss) include impaired physical and mental performance, increased risk for mental health disorders (such as, depression and substance abuse), and increased risk for medical diseases, including hypertension, diabetes, heart disease, and stroke.
Now, preliminary findings from a Penn Medicine study (abstract #0508) presented at SLEEP 2016, the 30th annual meeting of the Associated Professional Sleep Societies LLC, suggest that what may prevent 70 to 80 percent of individuals with new onset insomnia (acute insomnia) from developing chronic insomnia is a natural tendency to self-restrict time in bed (TIB). For example, if someone goes to sleep at 11 p.m. and wakes up at 5 a.m. (versus an intended 7:30 a.m.), they start their day, rather than lie awake in bed.
Electing to stay awake (rather than staying in bed trying to sleep) is not only a productive strategy for an individual with acute insomnia, but is also one that is formally deployed as part of cognitive behavioral therapy for chronic insomnia.
Last month, the American College of Physicians recommended Cognitive Behavioral Therapy (CBT) as the initial, first-line treatment for chronic insomnia, based on data showing the therapy can improve symptoms without the side effects associated with sleep drugs.
By evaluating over a year how time in bed varies in 416 individuals who remain good sleepers (GS), in good sleepers who begin suffering from acute insomnia and then recover (GS-AI-REC), and in good sleepers who transition to acute insomnia and then to long-term chronic insomnia (GS-AI-CI), the study provides the first evidence supporting the significant role that sleep extension – the effort to recover lost sleep by increasing one’s sleep opportunity, or TIB – plays in turning acute insomnia into chronic insomnia. The results from these preliminary data analyses show that 20 percent of the population of good sleepers experience acute insomnia per year, 45 percent of these individuals recover, 48 percent have persistent but periodic insomnia, and 7 percent develop chronic insomnia.
“Those with insomnia typically extend their sleep opportunity,” says Michael Perlis, PhD, an associate professor in Psychiatry and director of the Penn Behavioral Sleep Medicine Program. “They go to bed early, get out of bed late, and they nap. While this seems a reasonable thing to do, and may well be in the short term, the problem in the longer term is it creates a mismatch between the individual’s current sleep ability and their current sleep opportunity; this fuels insomnia.”
The findings offer the first data confirming a theory (the 3P model of insomnia) developed by the late Arthur Spielman in the 1980s, that says the catalyst for the transition from acute to chronic insomnia is “sleep extension,” that is, the tendency to expand sleep opportunity to make up for sleep loss.
Echoing Spielman, Perlis says, “Acute insomnia is likely a natural part of the human condition. If you think about the fight flight response, as trigger for sleeplessness, this makes sense. That is, it shouldn’t matter that it’s 3 a.m. and you’ve been awake for the last 22 hours, if you’re being threatened and you believe there is a threat to your quality of life or existence, it’s not a good time to sleep. It is understandable that sleeplessness has persisted as an adaptive response to such circumstances. In contrast, it’s hard to imagine how chronic insomnia is anything but bad…and the clinical research data support this position given chronic insomnia’s association with increased medical and psychiatric morbidity.”
Co-authors on the study include Ellis J. of the Northumbria Center for Sleep Research (United Kingdom), Knashawn H. Morales from Penn, Michael Grandner of the University of Arizona, and Charles Corbitt, Genevieve Nesom , and Waliuddin Khader from Penn. This work was funded by the National Institutes of Health (NIH R01AG041783) and the Economic Social Research Council (RES-061-25-0120-A).
Perlis will present the team’s findings at SLEEP on Wednesday June 15, 2016 at 9:30 am in room 605.
###Penn Medicine is one of the world's leading academic medical centers, dedicated to the related missions of medical education, biomedical research, and excellence in patient care. Penn Medicine consists of the Raymond and Ruth Perelman School of Medicine at the University of Pennsylvania(founded in 1765 as the nation's first medical school) and the University of Pennsylvania Health System, which together form a $5.3 billion enterprise.
The Perelman School of Medicine has been ranked among the top five medical schools in the United States for the past 18 years, according to U.S. News & World Report's survey of research-oriented medical schools. The School is consistently among the nation's top recipients of funding from the National Institutes of Health, with $373 million awarded in the 2015 fiscal year.
The University of Pennsylvania Health System's patient care facilities include: The Hospital of the University of Pennsylvania and Penn Presbyterian Medical Center -- which are recognized as one of the nation's top "Honor Roll" hospitals by U.S. News & World Report -- Chester County Hospital; Lancaster General Health; Penn Wissahickon Hospice; and Pennsylvania Hospital -- the nation's first hospital, founded in 1751. Additional affiliated inpatient care facilities and services throughout the Philadelphia region include Chestnut Hill Hospital and Good Shepherd Penn Partners, a partnership between Good Shepherd Rehabilitation Network and Penn Medicine.Penn Medicine is committed to improving lives and health through a variety of community-based programs and activities. In fiscal year 2015, Penn Medicine provided $253.3 million to benefit our community.
Newswise — BIRMINGHAM, Ala. –
In a first-of-its-kind national event focused on increasing organ donation, the White House announced today at the Organ Donation Summit that the University of Alabama at Birmingham Division of Transplantation will be part of two national efforts to increase access to organ transplants and reduce the number of patients awaiting kidney transplantation.
The endeavors, designed specifically to increase the number of living donor kidney transplants, will tailor a Live Donor Champion model for African-Americans and teach patients in need of transplant how to set up their Facebook page in the way that best tells their story to increase their chances of finding a living kidney donor.
“The institutional commitment UAB has made to the Division of Transplantation and the Comprehensive Transplant Institute and the ingenious work of our transplant team have cemented our transplant program as one of the best in the nation,” said Selwyn Vickers, M.D., senior vice present for Medicine and dean of UAB’s School of Medicine. “We have the ability to provide opportunities for lifesaving treatments beyond standard clinical techniques and have the infrastructure in place to properly educate and inform patients to give them opportunities for transplant that they may not have had just a few years ago. We are excited to support the White House transplantation efforts, and we will continue our mission to provide the best care in the world for our citizens right here in Alabama while at the same time striving to have an impact on health care across the country.”
The programsThe Live Donor Champion model for African-Americans is part of a comprehensive program to teach patients how to leverage their personal connections and social networks to raise awareness about the need for organ donors and to help identify potential live donor candidates. The UAB program will be known as the Living Donor Navigator Program, according to Michael Hanaway, M.D., surgical director of the Kidney Transplant Program, and Jayme Locke M.D., director of the Incompatible Kidney Transplant Program.
“African-Americans face a significantly higher incidence of end stage renal disease and disproportionately low rates of live donor transplantation, so the need in this community is real and vital,” said Locke, who will oversee the UAB program. “The Living Donor Navigator Program, which has been tested at Johns Hopkins University and other places, is associated with an over fivefold increase in identification of potential live donor candidates. We are excited to launch this program at UAB and hope we will see the same type of impact in the communities we serve.”
The Living Donor Navigator Program will help patients identify someone in their family who can be a Living Donor Champion. The person they identify will be trained by UAB on the donation process and how to approach potential donors for their loved one in need. Johns Hopkins University, Northwestern University and UAB will all lead different initiatives within the Live Donor Champion model.
In the second program, UAB will be part of a collaborative effort with Johns Hopkins University designed to help patients in need of live donor transplants leverage their social networks to find potential living kidney donors. The program will teach transplant patients how to use a specially designed Facebook app to share their story. The hope is that this will help those in need have a better opportunity to find a living donor. Locke, the co-principal investigator, says UAB patients in need of kidney transplants will begin participating in both programs by the end of the year.
“The UAB Department of Surgery is nationally and internationally known as one of the best departments in the country with strong clinical programs and a long history of making important contributions to the field, and this opportunity to support White House efforts to increase living transplant donation raises that bar even further,” said Herbert Chen, M.D., chair of the Department of Surgery and surgeon-in-chief at UAB Hospital. “This is an incredible opportunity for the people of Alabama and throughout the Southeast who are in need of a transplant. We are excited for what these programs can potentially do for them.”
Growing opportunities for patientsUAB transplant patients come from throughout Alabama, the southeast region, and across the United States.
“Our kidney program has performed more living donor transplants than any other program in the United States since 1987, and we are one of the three largest kidney-transplant centers in the nation,” said Devin Eckhoff, M.D., director of UAB’s Division of Transplantation. “Our experience performing kidney transplants from living donors ensures the highest level of care and better outcomes for our patients — both kidney donors and recipients.”
As far back as a decade ago, UAB’s kidney transplant program began laying the groundwork to build a paired exchange and incompatible transplant program that would help patients who are difficult to match. New technologies emerged that enabled researchers and clinicians to specifically define harmful antibodies that are present in many previously transplanted patients.
The result of this work has led to the world’s longest kidney transplant chain at UAB. Sixty-five people have been transplanted since the chain began in December 2013. Many patient stories have been chronicled online at www.uab.edu/kidneychain. The chain also has been covered by ABC News.
UAB also continues to lead national research efforts to ensure transplanted organs last as long as possible. Roslyn Mannon, M.D., director of research at the UAB Comprehensive Transplant Institute (CTI) and also a kidney transplant specialist, is among those leading investigative efforts to help patients keep transplanted organs permanently.
“Several therapies now used around the world to prevent transplant rejection were first offered to patients at UAB,” said Robert Gaston, M.D., executive director of UAB’s CTI. “The goal of our current research efforts goes beyond success in preventing rejection to include identifying treatments that allow transplanted kidneys to last the full lifetime of the recipient.”
If you are interested in living kidney donation, visit UAB Medicine and fill out the Living Kidney Donor Screening Form.
About UABKnown for its innovative and interdisciplinary approach to education at both the graduate and undergraduate levels, the University of Alabama at Birmingham is the state of Alabama’s largest employer and an internationally renowned research university and academic medical center; its professional schools and specialty patient-care programs are consistently ranked among the nation’s top 50. UAB’s Center for Clinical and Translational Science is advancing innovative discoveries for better health as a two-time recipient of the prestigious Center for Translational Science Award. Find more information at www.uab.edu and www.uabmedicine.org.
About the UAB School of MedicineWith more than 800 medical students and a faculty of more than 1,200, the School of Medicine at the University of Alabama at Birmingham is one of the premiere academic medical centers in the United States. UAB is among the top 20 schools in research funding from the National Institutes of Health and is routinely listed among the best in various national rankings. UAB’s Medical-Scientist Training Program (M.D.-Ph.D.), Rural Medical Scholars Program and Early Medical School Acceptance Program are a few of the innovations on campus that foster collaboration across a multitude of disciplines. As the educational arm of UAB Medicine, students and residents train in a world-class setting; UAB Hospital’s 1,200 beds places it in among the largest hospitals in the country. Doctoral students in UAB’s Graduate Biomedical Sciences Program participate in interdisciplinary thematic programs that integrate more than 25 departments and 20 research centers across UAB. At theUAB School of Medicine, we discover knowledge that changes your world.
About UAB MedicineUAB Medicine comprises the School of Medicine and the $3 billion UAB Health System that includes all of the University of Alabama at Birmingham’s patient-care activities and 2,300 licensed beds in six hospitals, one of which is UAB Hospital — the third-largest public hospital in the United States, winner of the Women's Choice award, and one of U.S. News and World Report’s Best Hospitals. UAB is the state of Alabama’s largest single employer and an internationally renowned research university and academic health center; its professional schools and specialty patient-care programs are consistently ranked among the nation’s top 50. UAB is the largest academic medical center in Alabama and one of the top four largest academic medical centers in the United States.
EDITOR’S NOTE: The University of Alabama at Birmingham is a separate, independent institution from the University of Alabama, which is located in Tuscaloosa. Please use University of Alabama at Birmingham on first reference and UAB on all subsequent references.
VIDEO: www.youtube.com/uabnews TEXT: www.uab.edu/news TWEETS: www.twitter.com/uabnews

Newswise —
Drexel University scientists have discovered an unusual mechanism for how two new antimalarial drugs operate: They give the parasite’s skin a boost in cholesterol, making it unable to traverse the narrow labyrinths of the human bloodstream. The drugs also seem to trick the parasite into reproducing prematurely.
Malaria is a mosquito-borne disease caused by Plasmodium parasites. After a person is bitten, the parasite invades the victim’s red blood cells. There, it eventually divides into daughter parasites, which continue to destroy each red blood cell they infect.
There are several drugs under development that interrupt this life cycle, including a class of compounds discovered in 2014 by Akhil Vaidya, PhD, a professor at Drexel University College of Medicine. In their 2014 study, Vaidya and his research team found that these drugs increase levels of sodium within the parasites’ cells, causing them to swell and erupt.
However, in a new study, published recently in PLOS Pathogens, the researchers have revealed that this sodium increase actually triggers a more complex cascade of events, eventually changing the parasite’s outer membrane and also tricking it into early reproduction, which renders the parasite inert.
“Nobody suspected something like this to be the mode of action,” said Vaidya, who also directs Drexel’s Center for Molecular Parasitology. “The mechanism is a lot more complicated and interesting than we originally thought.”
In this study, the scientists focused on two small-molecule drugs, one of which is undergoing clinical trials. Despite very different molecular structures, both drugs initially increase sodium within the parasite and subsequently kill the pathogen. Until now, scientists have not understood why the increase in sodium concentration leads to the malaria parasite’s demise.
To explore this question, the researchers first tested the properties of the Plasmodium plasma membrane — or the parasite’s outer skin — before and after exposure to antimalarial drugs. The Plasmodium membrane is unusual, because it contains very low levels of cholesterol, a major lipid component of most other membranes, including those of human red blood cells.
The Drexel scientists hypothesized that the low cholesterol content permits greater flexibility for the parasite to travel through the human bloodstream and to withstand the stress of blood circulation. They propose that the sodium increase, caused by the antimalarial drugs, somehow interferes with that elasticity.
The researchers used a cholesterol-dependent detergent to detect the presence of lipids in the parasite membrane. They found that indeed both drug treatments appeared to add a significant amount of cholesterol to the Plasmodium plasma membrane.
“We believe that the cholesterol makes the parasite rigid, and then the parasite can no longer pass through very small spaces in the bloodstream,” Vaidya said, adding that the parasite cannot continue its lifecycle if it cannot enter red blood cells.
Just two hours after treatment, the scientists also saw that many of the parasites showed fragmented nuclei and interior membranes, which are the precursors to cell division. But these changes happened without any sign that the parasite’s genome had multiplied — a step that is necessary for a cell to divide and survive.
The researchers hypothesize that sodium influx is a normal step during the malaria parasite’s division. The antimalarial drugs prematurely induce this signaling event, and the parasite begins dividing before it should.
“The parasite is not ready to divide yet, so it can not survive. It is like premature delivery of an infant,” Vaidya said. “This whole cascade of events is triggered by these drug treatments.”
Malaria is the world’s deadliest parasitic disease. It kills more than 300,000 people per year, according to the World Health Organization, and affects up to 300 million.
One of the biggest challenges for treating malaria is drug resistance. The drugs that are currently available are quickly losing their potency, so researchers are scrambling to develop stronger treatments.
By understanding exactly how new drug candidates stop malaria, Vaidya and his team aim to reveal more about the parasite’s vulnerabilities. This, they hope, will eventually lead to the creation of more effective drugs against the disease. Vaidya noted that the best defense against malaria will always be a combination of treatments.
“We want to find the best ways to keep new drugs effective as long as we can,” Vaidya said.
The study can be previewed by press before the embargo date at: http://www.blogs.plos.org/everyone/files/2016/05/ppat-12-5-Das.pdfThe study will become available publicly after the embargo lifts at this link: http://www.dx.plos.org/10.1371/journal.ppat.1005647

Newswise —
Being married could improve your likelihood of surviving a heart attack and is associated with reduced length of hospital stay, according to research presented at the British Cardiovascular Society (BCS) Conference in Manchester today (1).
The team – a collaboration between researchers at institutions including Aston Medical School and the University of East Anglia – found that married people were 14 per cent less likely to die after a heart attack than single people. Married people were also, on average, likely to spend two fewer days in hospital than single people.
The study was performed by the ACALM (Algorithm for Comorbidities, Associations, Length of stay and Mortality) Study Unit. The algorithm has compiled a one million patient dataset utilising Hospital Episode Statistics (HES) data (2) from the North of England. Researchers studied over 25,000 patients with a heart attack diagnosis that took place between January 2000 and March 2013.
There are 188,000 hospital episodes attributed to heart attack in the UK each year, which is around one every three minutes (3). Improvements in diagnosis and treatment driven by research mean that around 7 out of 10 people now survive a heart attack.
It is not clear from this research why married people are more likely to survive a heart attack but the researchers feel the findings emphasise the importance of physical and emotional support after the event. Although previous studies have linked marriage to improved heart attack outcomes, this is the first study to suggest that marital status affects how quickly heart attack patients are discharged.
Being discharged from hospital sooner could be financially beneficial to the NHS – the average cost per day for a patient to stay on a surgical ward is up to £400 and it is estimated that reducing length of stays in cardiology alone could save the NHS up to £9.8 million (4, 5). And shorter stays can benefit patients as they are associated with a lower risk of hospital-acquired infections (6).
The researchers feel the results show the need for doctors to consider the psychosocial effects of a heart attack, and consider them as a risk factor, when treating and managing the discharge of a patient.
Dr Nicholas D. Gollop, Clinical Research Fellow in Cardiology and presenting author from the University of East Anglia, said:
“Our results should not be a cause for concern for single people who have had a heart attack. But they should certainly be a reminder to the medical community of the importance of considering the support a heart attack survivor will get once they’re discharged.”
The researchers hope to expand the ACALM dataset in future studies, where they will look at longer term outcomes and consider the impact of marital status on other heart conditions such as heart failure and also evaluate the impact of potential interventions such as cardiac rehab. Dr Rahul Potluri, Founder of the ACALM Study Unit and Clinical Lecturer at Aston Medical School, said:
“Our approach has already helped us perform research investigating the relationship between mental and physical health, and health services research particularly looking at the weekend effect. Utilising and analysing large data sets is essential to improve our understanding of medical conditions and to improve management options for patients.
“By looking at how larger numbers of heart attack patients do over a longer period of time in future research, we may be able to see additional psychosocial benefits of marriage, which can be targeted to further guide patient care.”
Recently a survey of BHF supporters found that one in three (30 per cent) heart attack survivors has suffered with anxiety or depression (7).
Dr Mike Knapton, Associate Medical Director at the British Heart Foundation (BHF), said:
“A heart attack can have both devastating physical and psychological effects – most of which are hidden from the outside world. These findings suggest the support offered by spouse can have a beneficial effect on heart attack survivors, perhaps helping to minimise the impact of a heart attack. “When you have your heart attack, whether you’re married or not, it’s important to remember that you are not alone. Enrolling on a cardiac rehabilitation course, for example, will help you to recover physically, psychologically, and also help you to meet people with similar experiences, who know what you’ve been through. At the BHF we would encourage all heart attack survivors to do cardiac rehab.”
Cem Hilmi, 42, from Palmer’s Green in London, was rushed into hospital three years ago after collapsing in the kitchen. Cem’s support from his wife, Rosa, and the rest of his family has helped him to recover. Cem said:
“After feeling a bit unwell and some numbness in my arm, it turned out that I’d had at least three serious heart attacks and needed emergency surgery. I was a keen runner but after the heart attack I couldn’t even get up the stairs on my own. Your life changes in one instant.
“I was determined to physically get better, but the emotional impact was huge and at times seemed the greatest obstacle to my recovery. With support from family, particularly my wife, friends, my local cardiac rehabilitation team, and of course the BHF, I overcame the emotional and physical barriers. Six months after the heart attack, fully recovered, I was able to do a half marathon and take part in other events to raise money for the BHF.”
Newswise —
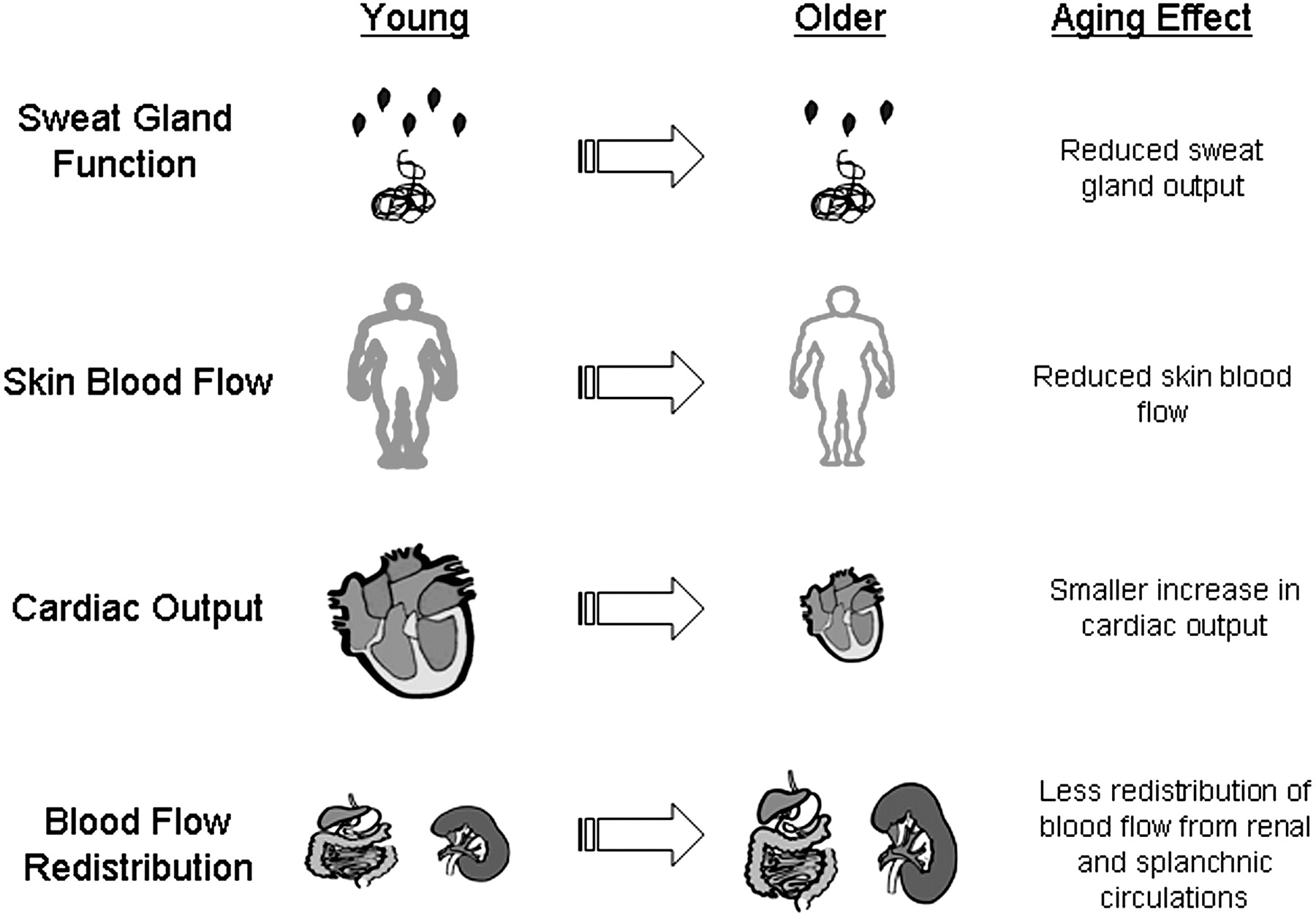
If you’re an older adult, a 30-minute workout may not be as effective, even at the cellular level, as it was when you were younger.
According to a new study, age may play a significant role in a cell’s ability to respond to that activity.
Tinna Traustadóttir of Northern Arizona University led the study, which was published in Free Radical Biology and Medicine, a journal of the Society for Redox Biology and Medicine.
In the study, a group of men ages 18 to 30 were tested against a group of older men 55 years and older. Study participants were generally healthy, non-smokers, who were not taking antioxidant supplements in excess of a multivitamin, or any non-steroidal anti-inflammatory drugs for two weeks leading up to the experiment.
The two groups cycled for 30-minutes, with blood being drawn six different times measuring cell function and antioxidant response. For this study, the exercise intensity was relative to the individual’s age and maximal aerobic capacity determined during a screening. “Through this study we were able to determine that an individual’s antioxidant response to exercise becomes suppressed with age,” said Traustadóttir an associate professor of biology. “Exercise is effective and critical for people of all ages, but this study shows that older adults do not achieve the same beneficial cellular responses as younger adults from a single bout of moderate exercise.”
The findings indicate a single session of submaximal aerobic exercise is sufficient to activate an important group of antioxidant genes at the whole cell level in both young and older adults. However, nuclear import of Nrf2, the regulator for this group of antioxidant genes, is impaired with aging. Nuclear import is required for Nrf2 to access the antioxidant gene targets. Together these data demonstrate for the first time the weakening of Nrf2 activity in response to exercise in older adults.
Traustadóttir’s ongoing research aims to identify molecular processes responsible for age-related cellular changes. By better understanding the molecular signals promoting beneficial effects of exercise, definitive recommendations could be made for improving the body’s reaction to oxidative stress, which could lower the risk for many chronic diseases.
Newswise — DURHAM, N.C. --
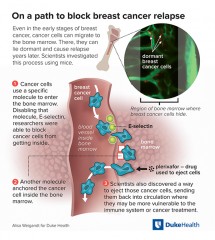
Scientists at the Duke Cancer Institute have identified a molecular key that breast cancer cells use to invade bone marrow in mice, where they may be protected from chemotherapy or hormonal therapies that could otherwise eradicate them.
Through years of experiments in mice, the scientists have found ways to outmaneuver this stealth tactic by not only preventing breast cancer cells from entering the bone marrow, but also by flushing cancer cells out into the blood stream where they could be targeted for destruction.
The findings provide insight into one of the most devastating tendencies of some breast cancers -- the ability to return after seemingly being vanquished. The researchers hope the findings, if replicated in additional animal and human tests, could eventually lead to new therapies for treating breast cancer.
“Clinical studies have found that breast cancer can be caught early and treated, and patients can have no signs of disease,” said Dorothy A. Sipkins, M.D., Ph.D., associate professor in the division of hematological malignancies and cellular therapy at Duke. “And then five, 10 or even 15 years later, a patient can relapse. Most often, the site of the metastasized cancer is in the bone.”
In an article published online May 25 in Science Translational Medicine, the researchers describe how cells from breast cancers that are hormone receptor-positive roam through the blood and tissues of mice. They’re hunting for specific blood vessels in bone marrow that contain the molecule E-selectin. With a key -- molecules on their surface that bind to E-selectin -- the cancer cells enter the spongy tissue inside bones, often lying dormant for years.
Hormone receptor-positive breast cancers are the most common type of breast cancer, according to the American Society of Clinical Oncology, and grow by exploiting the body’s estrogen or progesterone.
In human patients, these dormant cells can resurge later and create metastatic cancer relapse, for which there is no cure, said Sipkins, who is the paper’s senior author. Biopsies of bone marrow in human breast cancer patients have shown that even at very early stages of the cancer, roaming cancer cells, or micrometastases, are making their way out of the breast and into the bone marrow, Sipkins said.
“Now we know how they are getting in,” she said. “We also identified an important mechanism that allows them to remain anchored in the bone marrow. In the mouse, our findings could offer new strategies to intervene at the molecular level before dormant cells can take hold and cause relapse.”
One strategy is finding a way to inhibit E-selectin, which could limit the cancer’s ability to travel into the bone and resurge as metastatic cancer, she said. The scientists used an E-selectin inhibitor called GMI-1271, which is currently in human clinical trials. They found the compound successfully prevented the breast cancer cells from entering the bone marrow in mice.
Because microscopic metastases can spread to the bone marrow before patients are even diagnosed with breast cancer, the researchers also tested a strategy that appears to kick dormant breast cancer cells out of their safe house in the bone marrow and back into circulation. They gave the mice plerixafor, an agent used in human bone marrow donors to push stem cells into the bloodstream for harvesting.
The drug was able to force dormant breast cancer cells out of the bone tissue into the bloodstream. The researchers hypothesize that flushing these dormant cancer cells back into the bloodstream might give the immune system, chemotherapy or hormonal therapy another opportunity at killing them off, Sipkins said. She and colleagues hope to investigate that approach further.
“We are hopeful that by understanding how these breast cancer cells migrate through the body and what their life cycle is, we can discover ways to make them more vulnerable and treatable,” Sipkins said. “Our hope is to move forward with additional studies in mice to better understand our approach before moving on to studies in humans.”
In addition to Sipkins, study authors include lead author Trevor T. Price; Monika L. Burness; Ayelet Sivan; Matthew J. Warner; Renee Cheng; Clara H. Lee; Lindsey Olivere; Karrie Comatas; John Magnani; H. Kim Lyerly; Qing Cheng; and Chad M. McCall.The research was supported by the Young Investigator Award program of the American Society of Clinical Oncology, a Developmental Research Project Award from the University of Chicago Breast Cancer Specialized Program of Research Excellence AQ16, and the Duke Cancer Institute.
The authors cite one disclosure: John Magnani is vice president and chief scientific officer of GlycoMimetics Inc. GlycoMimetics has a patent for GMI-1271, which was used in the study to inhibit E-selectin in breast cancer cells.
###

Newswise —
According to a recent survey by FAIR Health, a nonprofit organization that gathers information on health data, more than 50 percent of millennials use means such as retail clinics, urgent care centers or emergency rooms for nonemergency medical care.
University of Alabama at Birmingham School of Medicine Associate Dean of Rural and Primary Care William Curry, M.D., says convenience is the main factor.
“Those care providers are convenient, and often they provide exactly the care someone needs,” Curry said. “It’s important to realize they cannot take the place of a primary care provider for the screening, prevention and long-term follow-up that we all need, customized to each of us.”
Curry says that generally healthy and busy younger people of every generation typically assume everything was fine as long as they felt good, but screening and preventive services have proved to be worthwhile at every age. He says millennials may have additional barriers to hearing and believing primary care is important.
“For one thing, medicine has oversold and misdirected some efforts, making skepticism understandable,” Curry said. “We have ‘medicalized’ so much that the volume of recommendations and warnings can lead to information overload and alarm fatigue.”
Millennials typically turn to Google and WebMD before visiting actual doctors, whom they are less likely to visit repeatedly or regularly.
“Millennials have grown up with the internet and great digital tools that bring libraries and opinions to their fingertips,” he said. “I see them sometimes assuming all that information is equally reliable when it is not.”
Curry says millennials sometimes believe they can find simpler, less demanding alternatives through the internet and a dietary regimen or natural remedy.
“These may be helpful or not, but they unfortunately can’t take the place of medical screening and prevention that has been proved effective,” he said. “The short solution is to have a healthy skepticism but to accept good evidence of value.”
Curry also believes a lack of primary care physicians is another reason millennials are less likely to seek one out.
“The shortages of primary care physicians are bad enough just from the lack of supply and the growth of the population,” Curry said. “With more people having insurance, demand for primary care services increases.”
He says Alabama has been more accommodating to shortages of primary care physicians for a much longer time compared to states like Massachusetts.
Why does it matter?
Curry says there are many advantages for millennials to find a primary care physician. He says seeing someone who knows you and has a baseline record is quicker — and there is less chance that something will be overlooked.
Curry says relationships matter, and patients are more likely to get the correct diagnoses and treatments if they have a primary care provider.
For those with a personal history of a chronic health problem or of a family history of problems that often are inherited, such as diabetes, high blood pressure, heart disease, stroke, high cholesterol, chronic lung disease, or others, it is especially important to have a primary care physician, regardless of age.
Everyone should be screened for certain disorders, many of which can be present without symptoms for years. Women should get cervical cancer screenings and vaccinations. If all is well, repeat checks can be as infrequent as every three to five years for people under the age of 30. These approaches can prevent avoidable complications such as heart attack, stroke, kidney failure or vision loss.
“Unfortunately, if people wait for symptoms, a lot of damage will have occurred,” Curry said.
What do I look for?
Curry says it is important to research when it comes to looking for a primary care physician.
“Find someone who is available and with whom you feel comfortable,” he said. “Check their profile for where they trained and whether they are board-certified. Do they have an internet patient portal to make communication easy for test results or questions? Are office hours a fit for your schedule? What kind of coverage is available from a partner or associate if your physician is out? Do they have nurse practitioners or physician assistants in the practice to improve access?”
He says, if possible, talk to someone with experience as a patient there, or check online comments or ratings; but keep in mind these ratings may not be entirely reliable.